Jennifer D Stowell, Ian Sue Wing, Yasmin Romitti, Patrick L Kinney, Gregory A Wellenius
{"title":"Emergency department visits in California associated with wildfire PM<sub>2.5</sub>: differing risk across individuals and communities.","authors":"Jennifer D Stowell, Ian Sue Wing, Yasmin Romitti, Patrick L Kinney, Gregory A Wellenius","doi":"10.1088/2752-5309/ad976d","DOIUrl":null,"url":null,"abstract":"<p><p>The threats to human health from wildfires and wildfire smoke (WFS) in the United States (US) are increasing due to continued climate change. A growing body of literature has documented important adverse health effects of WFS exposure, but there is insufficient evidence regarding how risk related to WFS exposure varies across individual or community level characteristics. To address this evidence gap, we utilized a large nationwide database of healthcare utilization claims for emergency department (ED) visits in California across multiple wildfire seasons (May through November, 2012-2019) and quantified the health impacts of fine particulate matter <2.5 <i>μ</i>m (PM<sub>2.5</sub>) air pollution attributable to WFS, overall and among subgroups of the population. We aggregated daily counts of ED visits to the level of the Zip Code Tabulation Area (ZCTA) and used a time-stratified case-crossover design and distributed lag non-linear models to estimate the association between WFS and relative risk of ED visits. We further assessed how the association with WFS varied across subgroups defined by age, race, social vulnerability, and residential air conditioning (AC) prevalence. Over a 7 day period, PM<sub>2.5</sub> from WFS was associated with elevated risk of ED visits for all causes (1.04% (0.32%, 1.71%)), non-accidental causes (2.93% (2.16%, 3.70%)), and respiratory disease (15.17% (12.86%, 17.52%)), but not with ED visits for cardiovascular diseases (1.06% (-1.88%, 4.08%)). Analysis across subgroups revealed potential differences in susceptibility by age, race, and AC prevalence, but not across subgroups defined by ZCTA-level Social Vulnerability Index scores. These results suggest that PM<sub>2.5</sub> from WFS is associated with higher rates of all cause, non-accidental, and respiratory ED visits with important heterogeneity across certain subgroups. Notably, lower availability of residential AC was associated with higher health risks related to wildfire activity.</p>","PeriodicalId":72938,"journal":{"name":"Environmental research, health : ERH","volume":"3 1","pages":"015002"},"PeriodicalIF":0.0000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11632356/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Environmental research, health : ERH","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1088/2752-5309/ad976d","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/11 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
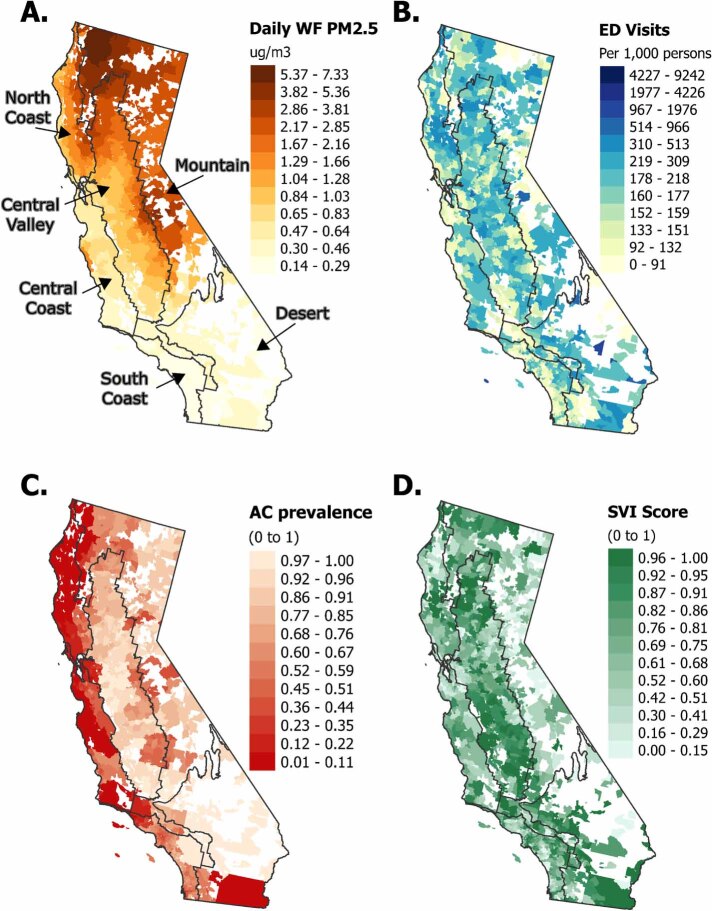
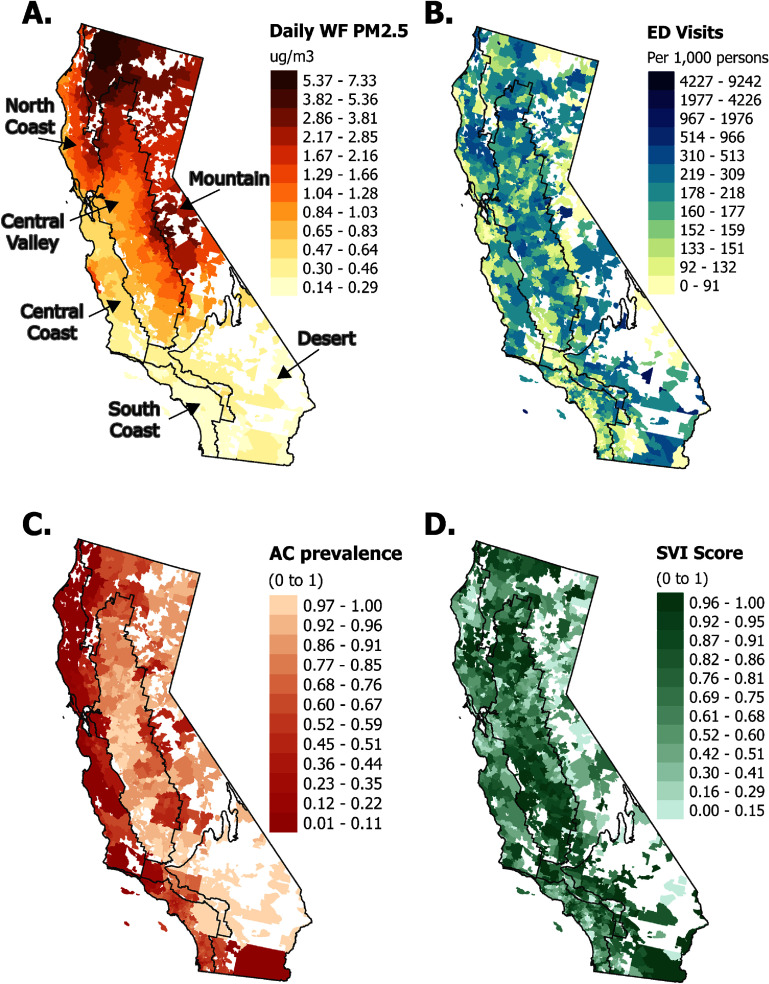
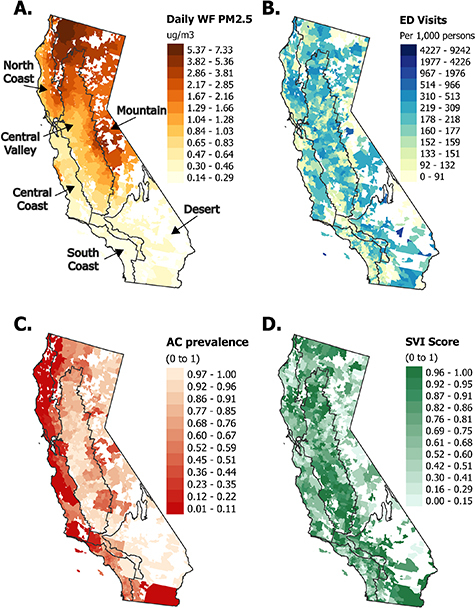
The threats to human health from wildfires and wildfire smoke (WFS) in the United States (US) are increasing due to continued climate change. A growing body of literature has documented important adverse health effects of WFS exposure, but there is insufficient evidence regarding how risk related to WFS exposure varies across individual or community level characteristics. To address this evidence gap, we utilized a large nationwide database of healthcare utilization claims for emergency department (ED) visits in California across multiple wildfire seasons (May through November, 2012-2019) and quantified the health impacts of fine particulate matter <2.5 μm (PM2.5) air pollution attributable to WFS, overall and among subgroups of the population. We aggregated daily counts of ED visits to the level of the Zip Code Tabulation Area (ZCTA) and used a time-stratified case-crossover design and distributed lag non-linear models to estimate the association between WFS and relative risk of ED visits. We further assessed how the association with WFS varied across subgroups defined by age, race, social vulnerability, and residential air conditioning (AC) prevalence. Over a 7 day period, PM2.5 from WFS was associated with elevated risk of ED visits for all causes (1.04% (0.32%, 1.71%)), non-accidental causes (2.93% (2.16%, 3.70%)), and respiratory disease (15.17% (12.86%, 17.52%)), but not with ED visits for cardiovascular diseases (1.06% (-1.88%, 4.08%)). Analysis across subgroups revealed potential differences in susceptibility by age, race, and AC prevalence, but not across subgroups defined by ZCTA-level Social Vulnerability Index scores. These results suggest that PM2.5 from WFS is associated with higher rates of all cause, non-accidental, and respiratory ED visits with important heterogeneity across certain subgroups. Notably, lower availability of residential AC was associated with higher health risks related to wildfire activity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


