{"title":"Dual antiplatelet versus alteplase in anterior and posterior circulation minor stroke.","authors":"Yu Cui, Hui-Sheng Chen","doi":"10.1136/svn-2024-003705","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The Antiplatelet versus R-tPA for Acute Mild Ischaemic Stroke trial has demonstrated the non-inferiority of dual antiplatelet therapy (DAPT) to alteplase in minor non-disabling stroke. This prespecified secondary analysis aimed to investigate whether the treatment effects were similar across stroke territories.</p><p><strong>Methods: </strong>Participants were divided according to stroke territory, which were subdivided into DAPT and alteplase. An excellent functional outcome at 90 days defined as modified Rankin Scale scoring 0-1 was primary outcome. National Institutes of Health Stroke Scale (NIHSS) score change and early neurological improvement measured by a 2-point decline in NIHSS score at 24 hours were secondary outcomes. Symptomatic intracerebral haemorrhage (sICH) and bleeding events were safety outcomes. Primary analyses adjusted unbalanced baseline characteristics between treatments by multivariate logistic regression.</p><p><strong>Results: </strong>A total of 719 patients were included: 566 in anterior circulation stroke (ACS) and 153 in posterior circulation stroke (PCS). Primary outcome was 94.1% in DAPT and 91.7% in alteplase among ACS patients (adjusted risk difference (RD) and 95% CI, 1.5% (-1.5% to 4.6%), p=0.32), while 91.2% in DAPT and 91.8% in alteplase among PCS patients (adjusted RD and 95% CI, -2.1% (-8.5% to 4.4%), p=0.53). Compared with alteplase, DAPT was associated with lower risk of sICH (p=0.03) and bleeding events (p<0.001) in ACS, but only lower risk of bleeding events (p=0.007) in PCS. Additionally, among ACS patients, the alteplase was superior to DAPT in terms of decrease in NIHSS score at 24 hours compared with admission (adjusted geometric mean ratio and 95% CI, -0.09 (-0.16 to -0.03), p=0.005) and early neurological improvement (adjusted RD and 95% CI, -7.2% (-11.6% to -2.7%), p=0.001).</p><p><strong>Conclusion: </strong>Among ischaemic stroke with minor non-disabling symptoms, DAPT was similar with intravenous alteplase regarding long-term functional outcome and better safety regardless of ACS or PCS. The potential benefit of intravenous alteplase regarding early neurological improvement in patients with ACS warrants further investigation.</p><p><strong>Trial registration number: </strong>NCT03661411.</p>","PeriodicalId":48733,"journal":{"name":"Journal of Investigative Medicine","volume":" ","pages":"491-498"},"PeriodicalIF":4.9000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415641/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Investigative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2024-003705","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: The Antiplatelet versus R-tPA for Acute Mild Ischaemic Stroke trial has demonstrated the non-inferiority of dual antiplatelet therapy (DAPT) to alteplase in minor non-disabling stroke. This prespecified secondary analysis aimed to investigate whether the treatment effects were similar across stroke territories.
Methods: Participants were divided according to stroke territory, which were subdivided into DAPT and alteplase. An excellent functional outcome at 90 days defined as modified Rankin Scale scoring 0-1 was primary outcome. National Institutes of Health Stroke Scale (NIHSS) score change and early neurological improvement measured by a 2-point decline in NIHSS score at 24 hours were secondary outcomes. Symptomatic intracerebral haemorrhage (sICH) and bleeding events were safety outcomes. Primary analyses adjusted unbalanced baseline characteristics between treatments by multivariate logistic regression.
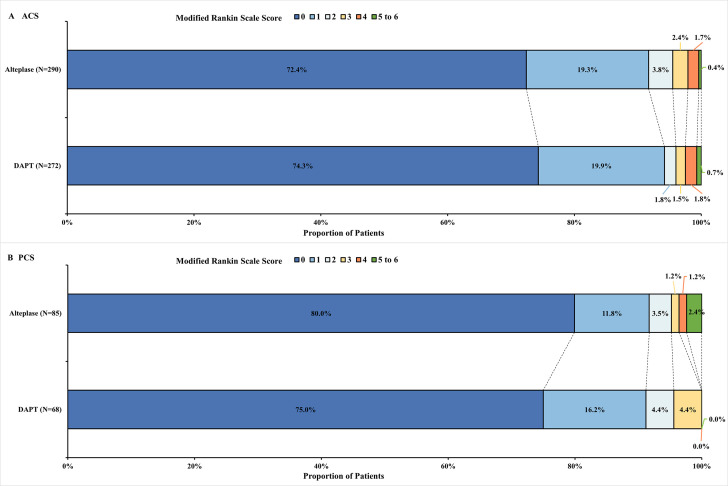
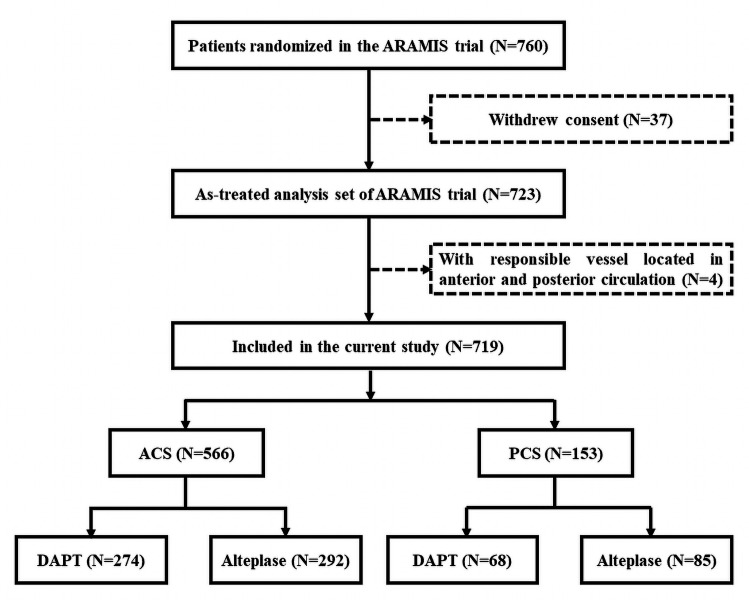
Results: A total of 719 patients were included: 566 in anterior circulation stroke (ACS) and 153 in posterior circulation stroke (PCS). Primary outcome was 94.1% in DAPT and 91.7% in alteplase among ACS patients (adjusted risk difference (RD) and 95% CI, 1.5% (-1.5% to 4.6%), p=0.32), while 91.2% in DAPT and 91.8% in alteplase among PCS patients (adjusted RD and 95% CI, -2.1% (-8.5% to 4.4%), p=0.53). Compared with alteplase, DAPT was associated with lower risk of sICH (p=0.03) and bleeding events (p<0.001) in ACS, but only lower risk of bleeding events (p=0.007) in PCS. Additionally, among ACS patients, the alteplase was superior to DAPT in terms of decrease in NIHSS score at 24 hours compared with admission (adjusted geometric mean ratio and 95% CI, -0.09 (-0.16 to -0.03), p=0.005) and early neurological improvement (adjusted RD and 95% CI, -7.2% (-11.6% to -2.7%), p=0.001).
Conclusion: Among ischaemic stroke with minor non-disabling symptoms, DAPT was similar with intravenous alteplase regarding long-term functional outcome and better safety regardless of ACS or PCS. The potential benefit of intravenous alteplase regarding early neurological improvement in patients with ACS warrants further investigation.
期刊介绍:
Journal of Investigative Medicine (JIM) is the official publication of the American Federation for Medical Research. The journal is peer-reviewed and publishes high-quality original articles and reviews in the areas of basic, clinical, and translational medical research.
JIM publishes on all topics and specialty areas that are critical to the conduct of the entire spectrum of biomedical research: from the translation of clinical observations at the bedside, to basic and animal research to clinical research and the implementation of innovative medical care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


