{"title":"Reduction of Ovarian Cysts After Endoscopic Surgery for Follicle-Stimulating Hormone-Producing Pituitary Adenoma.","authors":"Reo Ishii, Nozomi Harai, Tadatsugu Hosokawa, Ippei Tahara, Masakazu Ogiwara, Kyoichiro Tsuchiya","doi":"10.1210/jcemcr/luae231","DOIUrl":null,"url":null,"abstract":"<p><p>A 49-year-old woman presented with irregular menstrual bleeding, elevated estradiol (E2) (665 pg/mL [2441.21 pmol/L]) (reference range [RR]: menstrual period [MP] 20-50 pg/mL; 73.42-183.55 pmol/L), unsuppressed follicle-stimulating hormone (FSH) (19.3 mIU/mL [19.3 IU/L]) (RR: MP 3.5-10.0 mIU/mL; 3.5-10.0 IU/L), and cystic ovarian enlargement (right ovary, 109 mL; left ovary, 146 mL). A 7-mm pituitary microadenoma was also observed, and 6 months after referral, endoscopic transsphenoidal surgery was performed, resulting in a diagnosis of FSH-producing pituitary adenoma. Nine months postoperatively, the ovarian cysts had markedly shrunk. Although FSH-producing pituitary adenomas are rare, approximately 64% of nonfunctioning pituitary adenomas are positive for gonadotropin immunostaining. FSH-producing pituitary adenomas are often endocrinologically silent, with symptoms typically triggered by pituitary tumor enlargement. Early diagnosis can be facilitated by measuring FSH and E2 levels in cases of irregular vaginal bleeding, abnormal menstruation, ovarian enlargement, ovarian hyperstimulation syndrome, or infertility. If E2 is elevated but FSH is not suppressed, pituitary magnetic resonance imaging should be performed to identify FSH-producing pituitary adenomas. In cases of FSH-producing pituitary adenomas, including microadenomas, symptoms may improve after tumor resection, making surgery the preferred treatment option.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 12","pages":"luae231"},"PeriodicalIF":0.0000,"publicationDate":"2024-12-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11630798/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae231","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
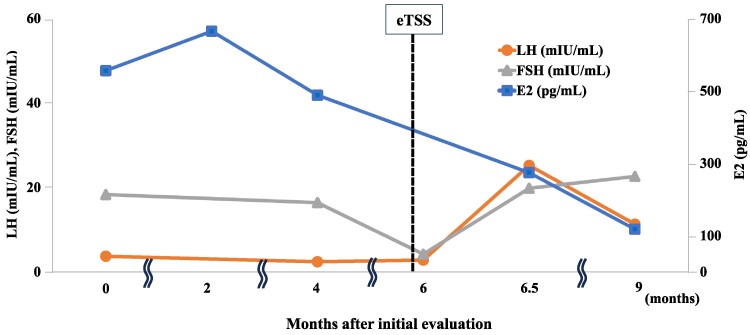
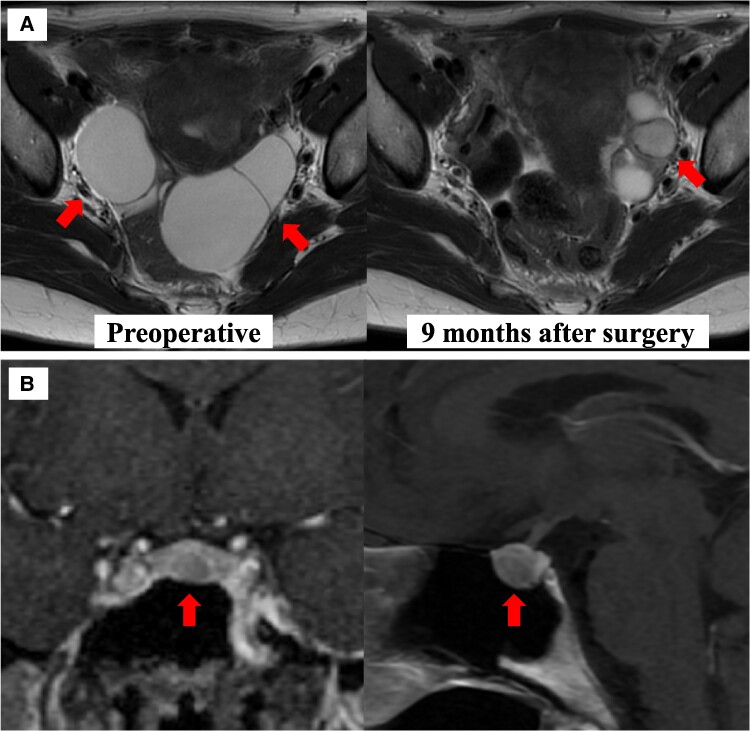
A 49-year-old woman presented with irregular menstrual bleeding, elevated estradiol (E2) (665 pg/mL [2441.21 pmol/L]) (reference range [RR]: menstrual period [MP] 20-50 pg/mL; 73.42-183.55 pmol/L), unsuppressed follicle-stimulating hormone (FSH) (19.3 mIU/mL [19.3 IU/L]) (RR: MP 3.5-10.0 mIU/mL; 3.5-10.0 IU/L), and cystic ovarian enlargement (right ovary, 109 mL; left ovary, 146 mL). A 7-mm pituitary microadenoma was also observed, and 6 months after referral, endoscopic transsphenoidal surgery was performed, resulting in a diagnosis of FSH-producing pituitary adenoma. Nine months postoperatively, the ovarian cysts had markedly shrunk. Although FSH-producing pituitary adenomas are rare, approximately 64% of nonfunctioning pituitary adenomas are positive for gonadotropin immunostaining. FSH-producing pituitary adenomas are often endocrinologically silent, with symptoms typically triggered by pituitary tumor enlargement. Early diagnosis can be facilitated by measuring FSH and E2 levels in cases of irregular vaginal bleeding, abnormal menstruation, ovarian enlargement, ovarian hyperstimulation syndrome, or infertility. If E2 is elevated but FSH is not suppressed, pituitary magnetic resonance imaging should be performed to identify FSH-producing pituitary adenomas. In cases of FSH-producing pituitary adenomas, including microadenomas, symptoms may improve after tumor resection, making surgery the preferred treatment option.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


