Nick Panay, Richard A Anderson, Amy Bennie, Marcelle Cedars, Melanie Davies, Carolyn Ee, Claus H Gravholt, Sophia Kalantaridou, Amanda Kallen, Kimberly Q Kim, Micheline Misrahi, Aya Mousa, Rossella E Nappi, Walter A Rocca, Xiangyan Ruan, Helena Teede, Nathalie Vermeulen, Elinor Vogt, Amanda J Vincent
{"title":"Evidence-based guideline: premature ovarian insufficiency<sup />.","authors":"Nick Panay, Richard A Anderson, Amy Bennie, Marcelle Cedars, Melanie Davies, Carolyn Ee, Claus H Gravholt, Sophia Kalantaridou, Amanda Kallen, Kimberly Q Kim, Micheline Misrahi, Aya Mousa, Rossella E Nappi, Walter A Rocca, Xiangyan Ruan, Helena Teede, Nathalie Vermeulen, Elinor Vogt, Amanda J Vincent","doi":"10.1093/hropen/hoae065","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>How should premature/primary ovarian insufficiency (POI) be diagnosed and managed based on the best available evidence from published literature?</p><p><strong>Summary answer: </strong>The current guideline provides 145 recommendations on symptoms, diagnosis, causation, sequelae, and treatment of POI.</p><p><strong>What is known already: </strong>Premature ovarian insufficiency (POI) presents a significant challenge to women's health, with far-reaching implications, both physically and emotionally. The potential implications include adverse effects on quality of life; fertility; and bone, cardiovascular, and cognitive health. Although hormone therapy (HT) can mitigate some of these effects, many questions still remain regarding the optimal management of POI.</p><p><strong>Study design size duration: </strong>The guideline was developed according to the structured methodology for development of ESHRE guidelines. Key questions were determined by a group of experts and informed by a scoping survey of women and health care professionals. Literature searches and assessments were then performed. Papers published up to 30 January 2024 and written in English were included in the guideline. An integrity review was conducted for the randomized controlled trials (RCTs) on POI included in the guideline.</p><p><strong>Participants/materials setting methods: </strong>Based on the collected evidence, recommendations were formulated and discussed within the guideline development group until consensus was reached. Women with lived experience of POI informed the recommendations in general, and particularly on those on provision of care. A stakeholder review was organized after finalization of the draft. The final version was approved by the guideline development group and the ESHRE Executive Committee.</p><p><strong>Main results and the role of chance: </strong>New data indicate a higher prevalence of POI, 3.5%, than was previously thought. This guideline aims to help health care professionals to apply best practice care for women with POI. The recent update of the POI guideline covers 40 clinical questions on diagnosis of the condition, the different sequelae, including bone, cardiovascular, neurological and sexual function, fertility and general well-being, and treatment options, including HT. The list of clinical questions was expanded from the previous iteration of the guideline (2015) based on the scoping survey and appreciation of emerging knowledge of POI. Questions were added on the role of anti-Müllerian hormone (AMH) in the diagnosis of POI, fertility preservation, muscle health, and specific considerations for HT in iatrogenic POI. Additionally, the topic on complementary treatments was extended with specific focus on non-hormonal treatments and lifestyle management options. Significant changes from the previous 2015 guideline include the recommendations that only one elevated FSH >25 IU is required for diagnosis of POI, and guidance that AMH testing, repeat FSH measurement, and/or AMH may be required where there is diagnostic uncertainty. Recommendations were also updated regarding genetic testing, estrogen doses and regimens, use of the combined oral contraceptive and testosterone therapy. Women with lived experience of POI informed the recommendations on provision of care.</p><p><strong>Limitations reasons for caution: </strong>The guideline describes different management options, but it must be acknowledged that for most of these options, supporting evidence is limited for POI.</p><p><strong>Wider implications of the findings: </strong>The guideline provides health care professionals with clear advice on best practice in POI care, based on the best evidence currently available. In addition, a list of research recommendations is provided to guide further studies in POI.</p><p><strong>Study funding/competing interests: </strong>The guideline was developed and funded by ESHRE, American Society for Reproductive Medicine (ASRM), Centre for Research Excellence in Women's Health in Reproduction Life (CRE-WHiRL), and International Menopause Society (IMS), covering expenses associated with the guideline meetings, literature searches, and dissemination of the guideline. The guideline group members did not receive payments. N.P. declared grants from Bayer Pharma (research and consultancy) and NIHR-research POISE; consulting fees from Abbott, Astellas, Bayer, Besins, Lawley, Mithra, Theramex, Viatris; honoraria from Astellas, Bayer, Besins, Gedeon Richter, Theramex, Viatris; support for attending meetings and/or travel from Astellas, Bayer, Theramex, Viatris; President, International Menopause Society, Medical Advisory Committee member, British Menopause Society, Patron Daisy Network. A.J.V. declared grants from Amgen Australia, Australian NHMRC, and Australian MRFF; consulting fees from IQ Fertility; honoraria from the Australasian Menopause Society; participation on a Data Safety Monitoring Board or Advisory Board of Astellas; Board Member of the International Menopause Society (2020 to current) and Past president of the Australasian Menopause Society (2017-2019); R.A.A. declared grants from Roche (Research support, to institution), and participation on a Data Safety Monitoring Board of Bayer. M.C. declared grants from NHI; payments or honoraria from Up-to-Date (as editor/reviewer); Board Member of American Society of Reproductive Medicine, and of American Gynecological and Obstetrical Society. M.D. declared (NIHR-HTA Reference Number: NIHR133461; NIHR-HTA Reference Number: NIHR128757; Action Medical Research and Borne: GN2818) consulting fees from a small personal medical practice, support for attending meetings and/or travel from ESHRE, Bayer and UCLH special Trustees; Participation on the Advisory Board of the British Menopause Society, UKSTORE project, the Progress Educational Trust, and the Turner Syndrome Support Society UK; Leadership or fiduciary roles in the British Fertility Society (Trustee), Elizabeth Garrett Anderson Hospital Charity (chair of Trustees), and the Essex Wynter charitable trust (Trustee). C.E. declared being Chair of a SIG from the Royal Australian College of General Practitioners Integrative Medicine Specific Interest Group and Program Lead for Next Practice Western Sydney Integrative Health. C.H.G. declared grants from Novo Nordisk Foundation (Nos. NNF15OC0016474 and NNF20OC0060610), sygesikringen danmark (No 2022-0189), and the Independent Research Fund Denmark (Nos. 0134-00406 and 0134-00130B); consulting fees from Novo Nordisk, Merck, and Astra Zeneca. S.K. declared grants from Roche diagnostics. A.K. declared grants from NIH R01 5R01HD101475; consulting fees as Medical Reviewer for Flo and for Healthline; honoraria as Medical Consultant for Summus; support for attending meetings from the Reproductive Scientist Development Program; Society for Reproductive Investigation Council Member and Society for Assisted Reproduction Registry/Validation Chair; R.E.N. declared consulting fees from Astellas, Bayer Pharma, Besins Healthcare, Fidia, Theramex; honoraria from Abbott, Astellas, Exeltis, Fidia, Gedeon Richter, Merck & Co, Novo Nordisk, Shionogi Limited, Theramex, Viatris; payment for expert testimony from Vichy Laboratories; Participation in Data Safety Monitoring Board of Advisory board from Astellas and Bayer Healthcare; President elect of the International Menopause Society (IMS). H.T. declared a grant from NHMRC Centre for Research Excellence for women's health in reproductive life. A.B. declared being chair of the Daisy Network Charity. The other authors have no conflicts of interest to declare.</p><p><strong>Disclaimer: </strong><i>This guideline represents the views of ESHRE, ASRM, CRE-WHiRL, and IMS, which were achieved after careful consideration of the scientific evidence available at the time of preparation. In the absence of scientific evidence on certain aspects, a consensus between the relevant stakeholders has been obtained. Adherence to these clinical practice guidelines does not guarantee a successful or specific outcome, nor does it establish a standard of care. Clinical practice guidelines do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type</i>. <i>The collaborating societies make no warranty, expressed or implied, regarding the clinical practice guidelines and specifically exclude any warranties of merchantability and fitness for a particular use or purpose</i>. <i>(Full disclaimer available at www.eshre.eu/guidelines</i>.<i>)</i>.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2024 4","pages":"hoae065"},"PeriodicalIF":11.1000,"publicationDate":"2024-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11631070/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoae065","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
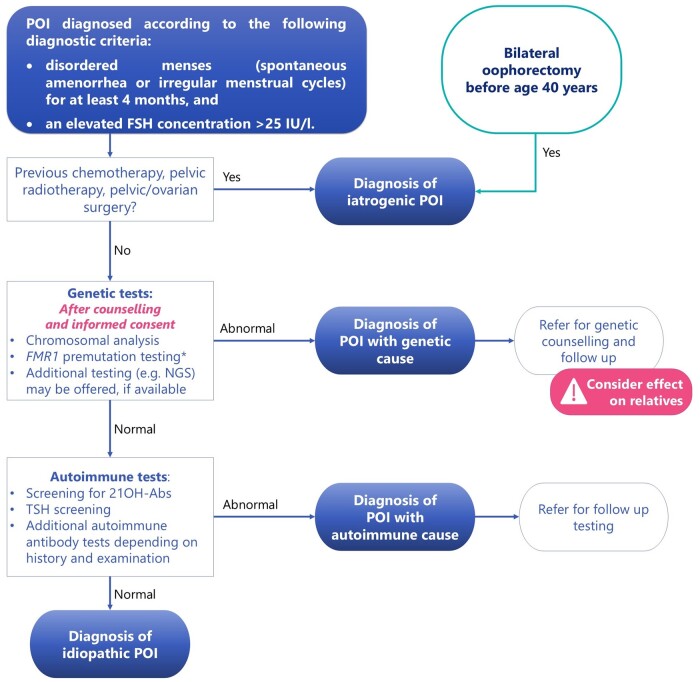
Study question: How should premature/primary ovarian insufficiency (POI) be diagnosed and managed based on the best available evidence from published literature?
Summary answer: The current guideline provides 145 recommendations on symptoms, diagnosis, causation, sequelae, and treatment of POI.
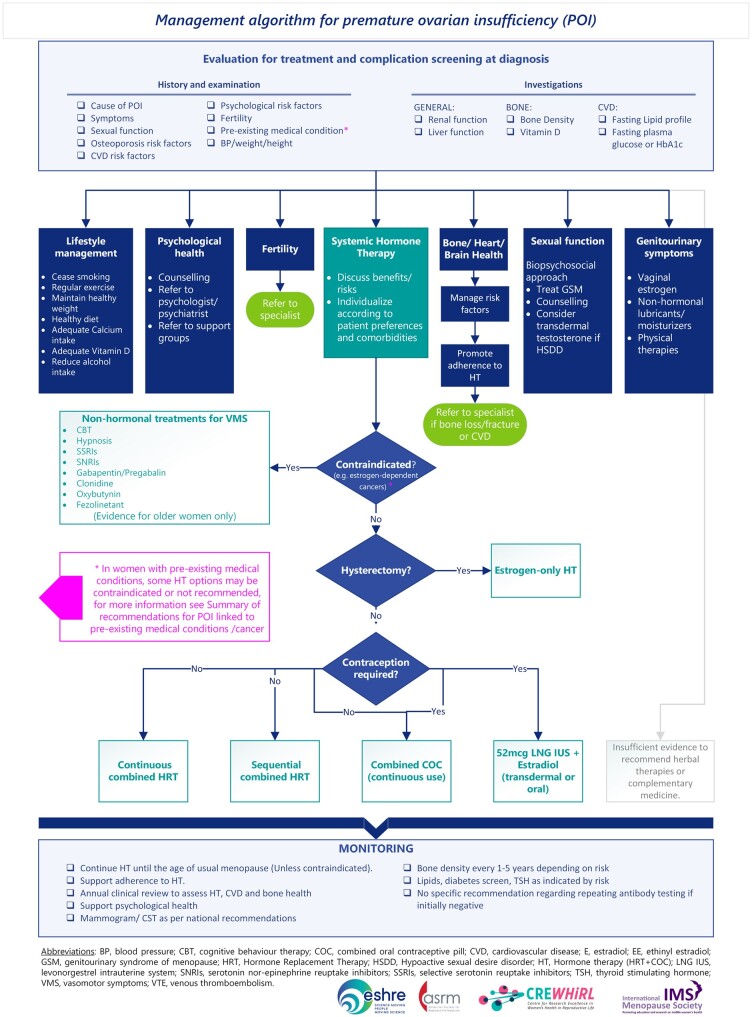
What is known already: Premature ovarian insufficiency (POI) presents a significant challenge to women's health, with far-reaching implications, both physically and emotionally. The potential implications include adverse effects on quality of life; fertility; and bone, cardiovascular, and cognitive health. Although hormone therapy (HT) can mitigate some of these effects, many questions still remain regarding the optimal management of POI.
Study design size duration: The guideline was developed according to the structured methodology for development of ESHRE guidelines. Key questions were determined by a group of experts and informed by a scoping survey of women and health care professionals. Literature searches and assessments were then performed. Papers published up to 30 January 2024 and written in English were included in the guideline. An integrity review was conducted for the randomized controlled trials (RCTs) on POI included in the guideline.
Participants/materials setting methods: Based on the collected evidence, recommendations were formulated and discussed within the guideline development group until consensus was reached. Women with lived experience of POI informed the recommendations in general, and particularly on those on provision of care. A stakeholder review was organized after finalization of the draft. The final version was approved by the guideline development group and the ESHRE Executive Committee.
Main results and the role of chance: New data indicate a higher prevalence of POI, 3.5%, than was previously thought. This guideline aims to help health care professionals to apply best practice care for women with POI. The recent update of the POI guideline covers 40 clinical questions on diagnosis of the condition, the different sequelae, including bone, cardiovascular, neurological and sexual function, fertility and general well-being, and treatment options, including HT. The list of clinical questions was expanded from the previous iteration of the guideline (2015) based on the scoping survey and appreciation of emerging knowledge of POI. Questions were added on the role of anti-Müllerian hormone (AMH) in the diagnosis of POI, fertility preservation, muscle health, and specific considerations for HT in iatrogenic POI. Additionally, the topic on complementary treatments was extended with specific focus on non-hormonal treatments and lifestyle management options. Significant changes from the previous 2015 guideline include the recommendations that only one elevated FSH >25 IU is required for diagnosis of POI, and guidance that AMH testing, repeat FSH measurement, and/or AMH may be required where there is diagnostic uncertainty. Recommendations were also updated regarding genetic testing, estrogen doses and regimens, use of the combined oral contraceptive and testosterone therapy. Women with lived experience of POI informed the recommendations on provision of care.
Limitations reasons for caution: The guideline describes different management options, but it must be acknowledged that for most of these options, supporting evidence is limited for POI.
Wider implications of the findings: The guideline provides health care professionals with clear advice on best practice in POI care, based on the best evidence currently available. In addition, a list of research recommendations is provided to guide further studies in POI.
Study funding/competing interests: The guideline was developed and funded by ESHRE, American Society for Reproductive Medicine (ASRM), Centre for Research Excellence in Women's Health in Reproduction Life (CRE-WHiRL), and International Menopause Society (IMS), covering expenses associated with the guideline meetings, literature searches, and dissemination of the guideline. The guideline group members did not receive payments. N.P. declared grants from Bayer Pharma (research and consultancy) and NIHR-research POISE; consulting fees from Abbott, Astellas, Bayer, Besins, Lawley, Mithra, Theramex, Viatris; honoraria from Astellas, Bayer, Besins, Gedeon Richter, Theramex, Viatris; support for attending meetings and/or travel from Astellas, Bayer, Theramex, Viatris; President, International Menopause Society, Medical Advisory Committee member, British Menopause Society, Patron Daisy Network. A.J.V. declared grants from Amgen Australia, Australian NHMRC, and Australian MRFF; consulting fees from IQ Fertility; honoraria from the Australasian Menopause Society; participation on a Data Safety Monitoring Board or Advisory Board of Astellas; Board Member of the International Menopause Society (2020 to current) and Past president of the Australasian Menopause Society (2017-2019); R.A.A. declared grants from Roche (Research support, to institution), and participation on a Data Safety Monitoring Board of Bayer. M.C. declared grants from NHI; payments or honoraria from Up-to-Date (as editor/reviewer); Board Member of American Society of Reproductive Medicine, and of American Gynecological and Obstetrical Society. M.D. declared (NIHR-HTA Reference Number: NIHR133461; NIHR-HTA Reference Number: NIHR128757; Action Medical Research and Borne: GN2818) consulting fees from a small personal medical practice, support for attending meetings and/or travel from ESHRE, Bayer and UCLH special Trustees; Participation on the Advisory Board of the British Menopause Society, UKSTORE project, the Progress Educational Trust, and the Turner Syndrome Support Society UK; Leadership or fiduciary roles in the British Fertility Society (Trustee), Elizabeth Garrett Anderson Hospital Charity (chair of Trustees), and the Essex Wynter charitable trust (Trustee). C.E. declared being Chair of a SIG from the Royal Australian College of General Practitioners Integrative Medicine Specific Interest Group and Program Lead for Next Practice Western Sydney Integrative Health. C.H.G. declared grants from Novo Nordisk Foundation (Nos. NNF15OC0016474 and NNF20OC0060610), sygesikringen danmark (No 2022-0189), and the Independent Research Fund Denmark (Nos. 0134-00406 and 0134-00130B); consulting fees from Novo Nordisk, Merck, and Astra Zeneca. S.K. declared grants from Roche diagnostics. A.K. declared grants from NIH R01 5R01HD101475; consulting fees as Medical Reviewer for Flo and for Healthline; honoraria as Medical Consultant for Summus; support for attending meetings from the Reproductive Scientist Development Program; Society for Reproductive Investigation Council Member and Society for Assisted Reproduction Registry/Validation Chair; R.E.N. declared consulting fees from Astellas, Bayer Pharma, Besins Healthcare, Fidia, Theramex; honoraria from Abbott, Astellas, Exeltis, Fidia, Gedeon Richter, Merck & Co, Novo Nordisk, Shionogi Limited, Theramex, Viatris; payment for expert testimony from Vichy Laboratories; Participation in Data Safety Monitoring Board of Advisory board from Astellas and Bayer Healthcare; President elect of the International Menopause Society (IMS). H.T. declared a grant from NHMRC Centre for Research Excellence for women's health in reproductive life. A.B. declared being chair of the Daisy Network Charity. The other authors have no conflicts of interest to declare.
Disclaimer: This guideline represents the views of ESHRE, ASRM, CRE-WHiRL, and IMS, which were achieved after careful consideration of the scientific evidence available at the time of preparation. In the absence of scientific evidence on certain aspects, a consensus between the relevant stakeholders has been obtained. Adherence to these clinical practice guidelines does not guarantee a successful or specific outcome, nor does it establish a standard of care. Clinical practice guidelines do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type. The collaborating societies make no warranty, expressed or implied, regarding the clinical practice guidelines and specifically exclude any warranties of merchantability and fitness for a particular use or purpose. (Full disclaimer available at www.eshre.eu/guidelines.).

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


