{"title":"A case of small intestinal fixation failure.","authors":"Kanako Oyanagi, Yosuke Horii, Hiroyuki Ishikawa, Kazuyasu Takizawa","doi":"10.1093/bjrcr/uaae046","DOIUrl":null,"url":null,"abstract":"<p><p>A 77-year-old woman underwent CT to evaluate haematemesis. The images showed that the third part of the duodenum flexed steeply on the right side of the aorta and ran caudally, without crossing anterior to the aorta. The duodenal-jejunal junction and jejunum were located on the patient's right side. Upper gastrointestinal endoscopy revealed a laceration at the gastric cardia, and a diagnosis of Mallory-Weiss syndrome was made. Repeat CT 7 days later revealed that the abnormal positioning of the intestinal tract had resolved spontaneously. Two months later, the patient experienced another episode of haematemesis, and CT revealed repeat deviation of the duodenal-jejunal junction and jejunum to her right side. Upper gastrointestinal endoscopy revealed another laceration at the gastric cardia, as in the previous study. On the basis of the initial CT findings showing the duodenal-jejunal junction in the right hemi-abdomen, intestinal malrotation was suspected. However, because the jejunum deviated repeatedly to the right side but resolved spontaneously, we diagnosed dysplasia of the ligament of Treitz. Laparotomy revealed a formed ligament of Treitz; however, fixation in the upper jejunum was incomplete. Additionally, CT revealed that the anterior pararenal space was loosely fixed and mobile. These factors may have caused the right-sided deviation of the small intestine. In this case, the third part of the duodenum likely flexed on the right side of the aorta, causing an obstruction that resulted in repeat vomiting episodes and Mallory-Weiss syndrome.</p>","PeriodicalId":45216,"journal":{"name":"BJR Case Reports","volume":"10 6","pages":"uaae046"},"PeriodicalIF":0.5000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11631180/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJR Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/bjrcr/uaae046","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
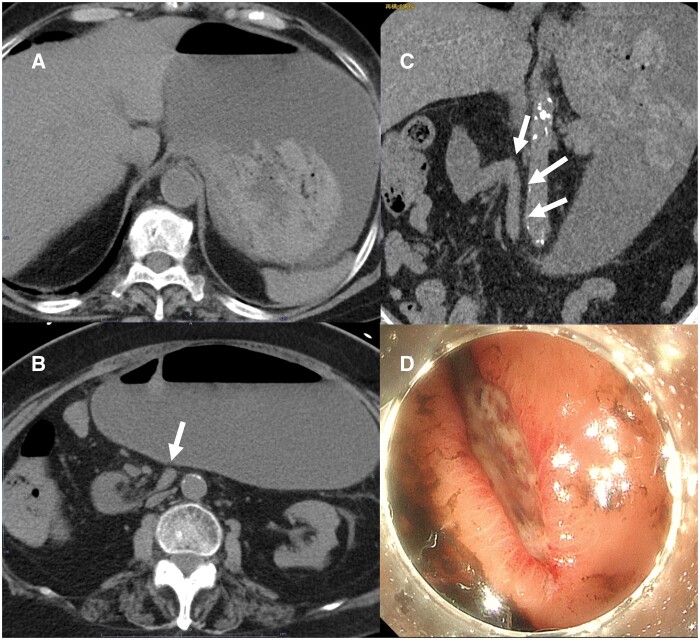
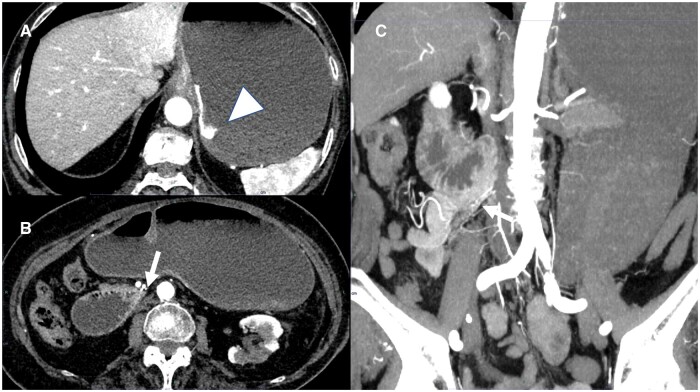
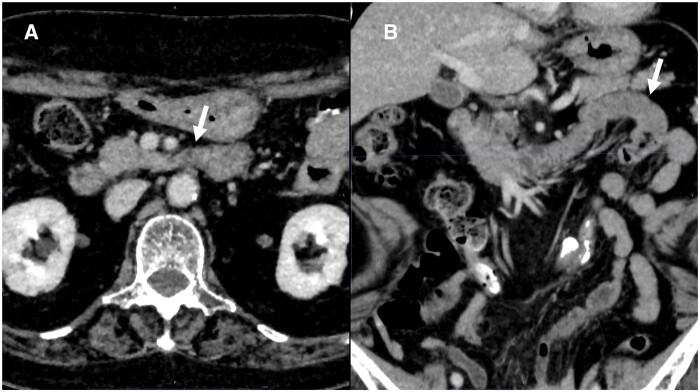
A 77-year-old woman underwent CT to evaluate haematemesis. The images showed that the third part of the duodenum flexed steeply on the right side of the aorta and ran caudally, without crossing anterior to the aorta. The duodenal-jejunal junction and jejunum were located on the patient's right side. Upper gastrointestinal endoscopy revealed a laceration at the gastric cardia, and a diagnosis of Mallory-Weiss syndrome was made. Repeat CT 7 days later revealed that the abnormal positioning of the intestinal tract had resolved spontaneously. Two months later, the patient experienced another episode of haematemesis, and CT revealed repeat deviation of the duodenal-jejunal junction and jejunum to her right side. Upper gastrointestinal endoscopy revealed another laceration at the gastric cardia, as in the previous study. On the basis of the initial CT findings showing the duodenal-jejunal junction in the right hemi-abdomen, intestinal malrotation was suspected. However, because the jejunum deviated repeatedly to the right side but resolved spontaneously, we diagnosed dysplasia of the ligament of Treitz. Laparotomy revealed a formed ligament of Treitz; however, fixation in the upper jejunum was incomplete. Additionally, CT revealed that the anterior pararenal space was loosely fixed and mobile. These factors may have caused the right-sided deviation of the small intestine. In this case, the third part of the duodenum likely flexed on the right side of the aorta, causing an obstruction that resulted in repeat vomiting episodes and Mallory-Weiss syndrome.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


