Felix N von Brackel, Jonathan Grambeck, Florian Barvencik, Michael Amling, Ralf Oheim
{"title":"In-depth clinical characterization of intravenous iron infusion-induced hypophosphatemic osteomalacia and its resolution.","authors":"Felix N von Brackel, Jonathan Grambeck, Florian Barvencik, Michael Amling, Ralf Oheim","doi":"10.1093/jbmrpl/ziae139","DOIUrl":null,"url":null,"abstract":"<p><p>Iron deficiency anemia is treated by iron supplementation. Increasing evidence has shown that the carbohydrate components in iron infusions can cause hypophosphatemia and subsequent osteomalacia due to excess intact fibroblast growth factor 23 (iFGF23). We here undertook an in-depth characterization of 13 patients with iron infusion-induced osteomalacia (IIIO). Patients were characterized (monocentric institutional practice) by means of laboratory, bone density, HR-pQCT, and virtual osteoid volume estimation. We additionally report a patient who was treated with burosumab because iron infusions had to be continued despite osteomalacia. All 13 patients received ferric carboxymaltose (FCM) infusions and presented with low phosphate levels. Stopping the FCM infusions and supportive treatment by substitution of phosphate, calcium, native, and/or active Vitamin D was the chosen therapeutic approach. Pain, mobility, and biochemical data, such as serum phosphate levels, BMD, bone microstructure, and virtual osteoid volume, were the main outcome measures. Our results indicate biochemical normalization (eg, phosphate levels pre: 0.50 mmol/L ± 0.23 mmol/L, post: 0.93 mmol/L ± 0.32 mmol/L, <i>p</i><.001) after stopping the FCM infusion and establishing supportive treatment. Additionally, pain levels on the visual analog scale (VAS) decreased (VAS<sub>pre</sub> 7.31 ± 1.22, VAS<sub>post</sub> 2.73 ± 1.27, <i>p</i><.0001) and areal BMD (expressed by T-score) improved significantly (T-score<sub>pre</sub>: -1.85 ± 1.84, T-score<sub>post</sub>: -0.91 ± 2.13, <i>p</i><.05). One patient requiring ongoing FCM infusions experienced significant additional benefits from burosumab treatment. In conclusion, our results highlight the importance of monitoring phosphate in patients treated with FCM infusions. Stopping FCM infusions is effective in addressing the excess of iFGF23 and thereby phosphate wasting. Supportive therapy enables quick recovery of the musculoskeletal system and improves pain levels in these patients.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 12","pages":"ziae139"},"PeriodicalIF":2.4000,"publicationDate":"2024-11-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11631080/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
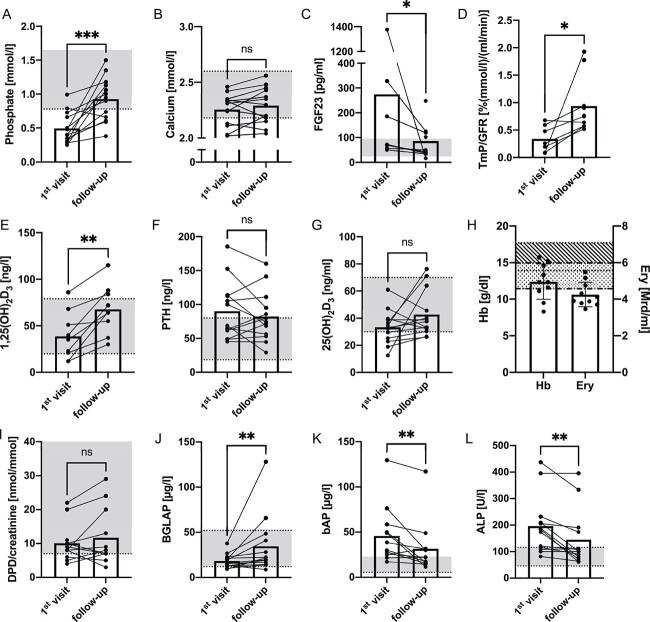
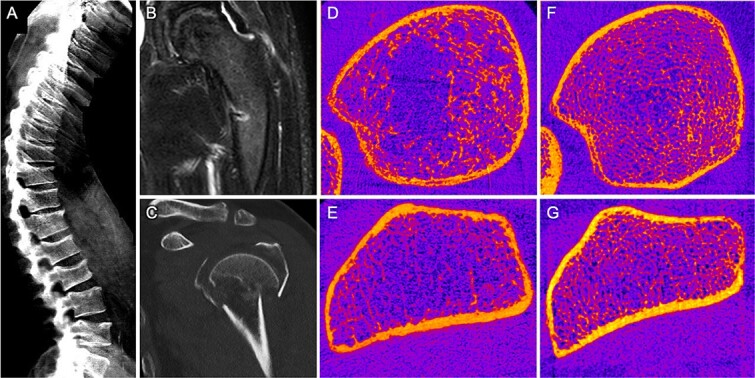
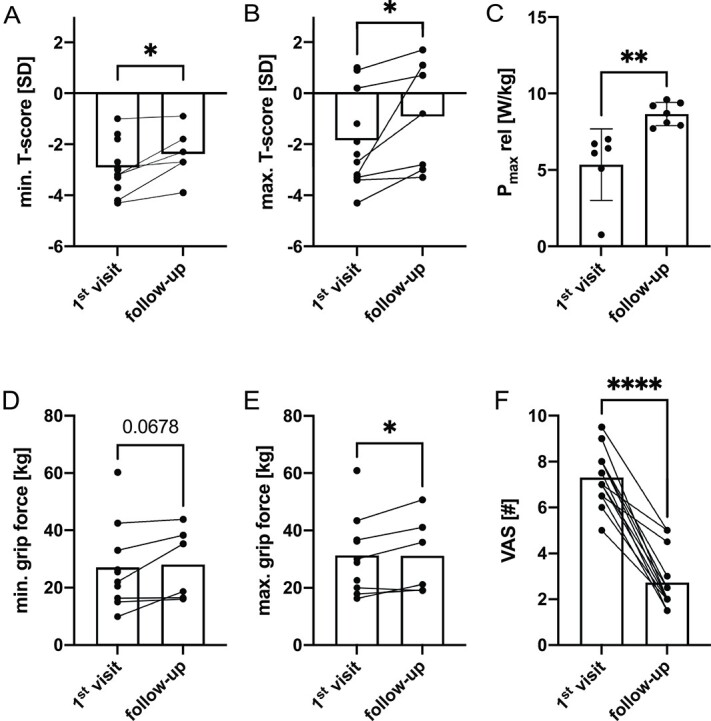
Iron deficiency anemia is treated by iron supplementation. Increasing evidence has shown that the carbohydrate components in iron infusions can cause hypophosphatemia and subsequent osteomalacia due to excess intact fibroblast growth factor 23 (iFGF23). We here undertook an in-depth characterization of 13 patients with iron infusion-induced osteomalacia (IIIO). Patients were characterized (monocentric institutional practice) by means of laboratory, bone density, HR-pQCT, and virtual osteoid volume estimation. We additionally report a patient who was treated with burosumab because iron infusions had to be continued despite osteomalacia. All 13 patients received ferric carboxymaltose (FCM) infusions and presented with low phosphate levels. Stopping the FCM infusions and supportive treatment by substitution of phosphate, calcium, native, and/or active Vitamin D was the chosen therapeutic approach. Pain, mobility, and biochemical data, such as serum phosphate levels, BMD, bone microstructure, and virtual osteoid volume, were the main outcome measures. Our results indicate biochemical normalization (eg, phosphate levels pre: 0.50 mmol/L ± 0.23 mmol/L, post: 0.93 mmol/L ± 0.32 mmol/L, p<.001) after stopping the FCM infusion and establishing supportive treatment. Additionally, pain levels on the visual analog scale (VAS) decreased (VASpre 7.31 ± 1.22, VASpost 2.73 ± 1.27, p<.0001) and areal BMD (expressed by T-score) improved significantly (T-scorepre: -1.85 ± 1.84, T-scorepost: -0.91 ± 2.13, p<.05). One patient requiring ongoing FCM infusions experienced significant additional benefits from burosumab treatment. In conclusion, our results highlight the importance of monitoring phosphate in patients treated with FCM infusions. Stopping FCM infusions is effective in addressing the excess of iFGF23 and thereby phosphate wasting. Supportive therapy enables quick recovery of the musculoskeletal system and improves pain levels in these patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


