{"title":"Histopathological Patterns of Cutaneous and Mucocutaneous Leishmaniasis Due to <i>L. aethiopica</i>.","authors":"Abay Atnafu, Zewditu Chanyalew, Sofia Yimam, Meaza Zeleke, Shimelis Negussie, Selfu Girma, Aklilu Melaku, Menberework Chanyalew","doi":"10.1155/drp/5267606","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Cutaneous leishmaniasis (CL) is an endemic disease in Ethiopia, mainly caused by <i>L. aethiopica</i>. Limited reports are available related to histopathological features of the skin lesion caused by <i>L. aethiopica</i>. This study aimed to analyze the histopathological features of CL due to <i>L. aethiopica</i>. <b>Materials and Methods:</b> A similar cohort polymerase chain reaction (PCR) confirmed CL patients from a previous own study, who were prospectively enrolled from All Africa Leprosy, Tuberculosis and Rehabilitation Training (ALERT) Hospital Addis Ababa, Kela Health Center in Gurage Zone, Siliti Health Center in Silit zone of southern nations and nationalities, as well as Ankober Health Center in Amhara region was used for data analysis. The histopathology was analyzed by performing hematoxylin and eosin (H&E) staining to look for the presence of general and specific histopathology patterns of the disease. Descriptive statistics was utilized using SPSS version 26.0 (SPSS, Inc., Chicago, United States of America). <b>Results:</b> Amastigotes were observed in skin biopsies of 29% (<i>n</i> = 2) mucocutaneous leishmaniasis (MCL) and 58% (<i>n</i> = 6) localized cutaneous leishmaniasis (LCL) patients. Diffused inflammatory cell infiltrate was observed in the dermal compartment of 77% (<i>n</i> = 20) samples while the remaining 23% (<i>n</i> = 6) had patchy or nodular inflammatory cell infiltrate. The dominant type of inflammatory cell infiltrate in the dermal compartments is macrophages and lymphocytes with a similar proportion, 23/26 (88.5%), followed by plasma cells, 21/26 (80.8%). Among all cases, 38.5% (<i>n</i> = 10) of them were categorized under the Type I pattern while Types IV and V patterns were reported in 26.9% (<i>n</i> = 7) and 34.6% (<i>n</i> = 9) of the remaining samples, respectively. The study found statistically significant correlations between necrosis and MCL (<i>p</i>=0.01), unorganized granulomas and LCL (<i>p</i>=0.04), and the presence of eosinophils and giant cell Langerhans with MCL (<i>p</i>=0.002 and <i>p</i> < 0.001, respectively). <b>Conclusion:</b> In our study, the histopathological patterns of the CL caused by <i>L. aethiopica</i> were shown to have a dermal change that was characterized by a domination of diffused inflammatory cell infiltrate. Most of the cell types in the infiltrate were macrophages and lymphocytes. In addition, amastigote resided in the histiocyte with a varying degree of intensity, and both the organized and unorganized granulomas were shown with a considerable proportion.</p>","PeriodicalId":11338,"journal":{"name":"Dermatology Research and Practice","volume":"2024 ","pages":"5267606"},"PeriodicalIF":1.9000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11623993/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Dermatology Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/drp/5267606","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
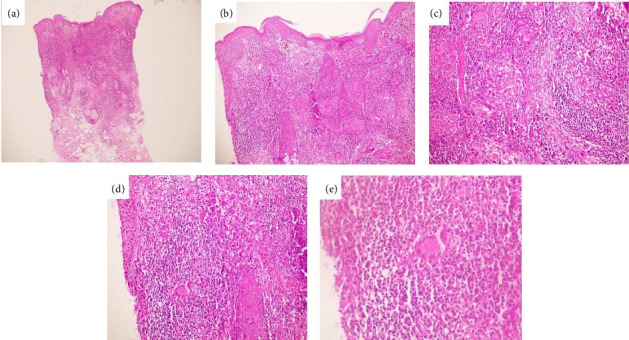
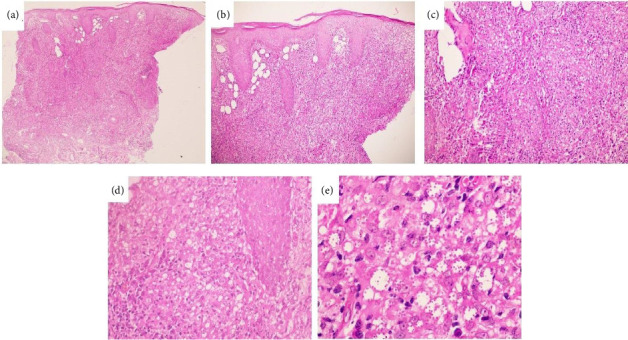
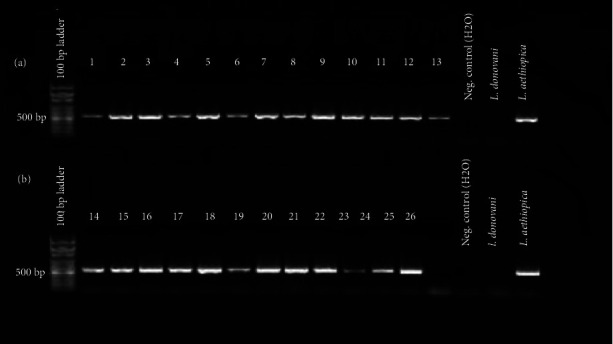
Background: Cutaneous leishmaniasis (CL) is an endemic disease in Ethiopia, mainly caused by L. aethiopica. Limited reports are available related to histopathological features of the skin lesion caused by L. aethiopica. This study aimed to analyze the histopathological features of CL due to L. aethiopica. Materials and Methods: A similar cohort polymerase chain reaction (PCR) confirmed CL patients from a previous own study, who were prospectively enrolled from All Africa Leprosy, Tuberculosis and Rehabilitation Training (ALERT) Hospital Addis Ababa, Kela Health Center in Gurage Zone, Siliti Health Center in Silit zone of southern nations and nationalities, as well as Ankober Health Center in Amhara region was used for data analysis. The histopathology was analyzed by performing hematoxylin and eosin (H&E) staining to look for the presence of general and specific histopathology patterns of the disease. Descriptive statistics was utilized using SPSS version 26.0 (SPSS, Inc., Chicago, United States of America). Results: Amastigotes were observed in skin biopsies of 29% (n = 2) mucocutaneous leishmaniasis (MCL) and 58% (n = 6) localized cutaneous leishmaniasis (LCL) patients. Diffused inflammatory cell infiltrate was observed in the dermal compartment of 77% (n = 20) samples while the remaining 23% (n = 6) had patchy or nodular inflammatory cell infiltrate. The dominant type of inflammatory cell infiltrate in the dermal compartments is macrophages and lymphocytes with a similar proportion, 23/26 (88.5%), followed by plasma cells, 21/26 (80.8%). Among all cases, 38.5% (n = 10) of them were categorized under the Type I pattern while Types IV and V patterns were reported in 26.9% (n = 7) and 34.6% (n = 9) of the remaining samples, respectively. The study found statistically significant correlations between necrosis and MCL (p=0.01), unorganized granulomas and LCL (p=0.04), and the presence of eosinophils and giant cell Langerhans with MCL (p=0.002 and p < 0.001, respectively). Conclusion: In our study, the histopathological patterns of the CL caused by L. aethiopica were shown to have a dermal change that was characterized by a domination of diffused inflammatory cell infiltrate. Most of the cell types in the infiltrate were macrophages and lymphocytes. In addition, amastigote resided in the histiocyte with a varying degree of intensity, and both the organized and unorganized granulomas were shown with a considerable proportion.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


