Artificial intelligence after the bedside: co-design of AI-based clinical informatics workflows to routinely analyse patient-reported experience measures in hospitals.
Oliver J Canfell, Wilkin Chan, Jason D Pole, Teyl Engstrom, Tim Saul, Jacqueline Daly, Clair Sullivan
{"title":"Artificial intelligence after the bedside: co-design of AI-based clinical informatics workflows to routinely analyse patient-reported experience measures in hospitals.","authors":"Oliver J Canfell, Wilkin Chan, Jason D Pole, Teyl Engstrom, Tim Saul, Jacqueline Daly, Clair Sullivan","doi":"10.1136/bmjhci-2024-101124","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To co-design artificial intelligence (AI)-based clinical informatics workflows to routinely analyse patient-reported experience measures (PREMs) in hospitals.</p><p><strong>Methods: </strong>The context was public hospitals (n=114) and health services (n=16) in a large state in Australia serving a population of ~5 million. We conducted a participatory action research study with multidisciplinary healthcare professionals, managers, data analysts, consumer representatives and industry professionals (n=16) across three phases: (1) defining the problem, (2) current workflow and co-designing a future workflow and (3) developing proof-of-concept AI-based workflows. Co-designed workflows were deductively mapped to a validated feasibility framework to inform future clinical piloting. Qualitative data underwent inductive thematic analysis.</p><p><strong>Results: </strong>Between 2020 and 2022 (n=16 health services), 175 282 PREMs inpatient surveys received 23 982 open-ended responses (mean response rate, 13.7%). Existing PREMs workflows were problematic due to overwhelming data volume, analytical limitations, poor integration with health service workflows and inequitable resource distribution. Three potential semiautomated, AI-based (unsupervised machine learning) workflows were developed to address the identified problems: (1) no code (simple reports, no analytics), (2) low code (PowerBI dashboard, descriptive analytics) and (3) high code (Power BI dashboard, descriptive analytics, clinical unit-level interactive reporting).</p><p><strong>Discussion: </strong>The manual analysis of free-text PREMs data is laborious and difficult at scale. Automating analysis with AI could sharpen the focus on consumer input and accelerate quality improvement cycles in hospitals. Future research should investigate how AI-based workflows impact healthcare quality and safety.</p><p><strong>Conclusion: </strong>AI-based clinical informatics workflows to routinely analyse free-text PREMs data were co-designed with multidisciplinary end-users and are ready for clinical piloting.</p>","PeriodicalId":9050,"journal":{"name":"BMJ Health & Care Informatics","volume":"31 1","pages":""},"PeriodicalIF":4.4000,"publicationDate":"2024-12-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11628959/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Health & Care Informatics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjhci-2024-101124","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To co-design artificial intelligence (AI)-based clinical informatics workflows to routinely analyse patient-reported experience measures (PREMs) in hospitals.
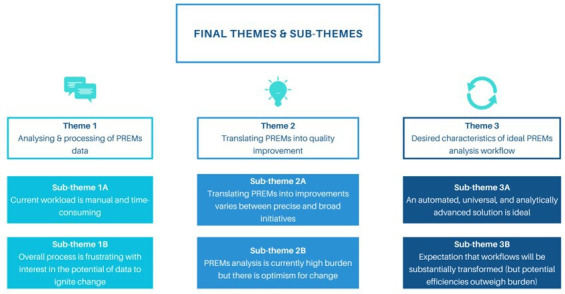
Methods: The context was public hospitals (n=114) and health services (n=16) in a large state in Australia serving a population of ~5 million. We conducted a participatory action research study with multidisciplinary healthcare professionals, managers, data analysts, consumer representatives and industry professionals (n=16) across three phases: (1) defining the problem, (2) current workflow and co-designing a future workflow and (3) developing proof-of-concept AI-based workflows. Co-designed workflows were deductively mapped to a validated feasibility framework to inform future clinical piloting. Qualitative data underwent inductive thematic analysis.
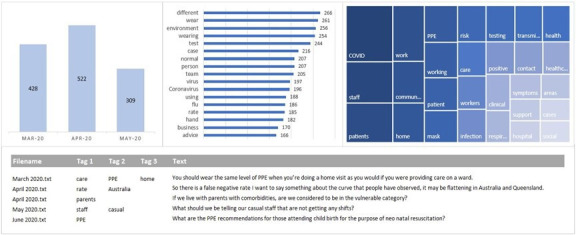
Results: Between 2020 and 2022 (n=16 health services), 175 282 PREMs inpatient surveys received 23 982 open-ended responses (mean response rate, 13.7%). Existing PREMs workflows were problematic due to overwhelming data volume, analytical limitations, poor integration with health service workflows and inequitable resource distribution. Three potential semiautomated, AI-based (unsupervised machine learning) workflows were developed to address the identified problems: (1) no code (simple reports, no analytics), (2) low code (PowerBI dashboard, descriptive analytics) and (3) high code (Power BI dashboard, descriptive analytics, clinical unit-level interactive reporting).
Discussion: The manual analysis of free-text PREMs data is laborious and difficult at scale. Automating analysis with AI could sharpen the focus on consumer input and accelerate quality improvement cycles in hospitals. Future research should investigate how AI-based workflows impact healthcare quality and safety.
Conclusion: AI-based clinical informatics workflows to routinely analyse free-text PREMs data were co-designed with multidisciplinary end-users and are ready for clinical piloting.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


