Cardiac Sympathetic Nerve Function in Patients with Severe Aortic Stenosis Prior and After Transcatheter Aortic Valve Implantation: Evaluation by 5-Year Risk Model.
{"title":"Cardiac Sympathetic Nerve Function in Patients with Severe Aortic Stenosis Prior and After Transcatheter Aortic Valve Implantation: Evaluation by 5-Year Risk Model.","authors":"Ryuta Egi, Kenji Fukushima, Yohji Matsusaka, Tomohiko Yamane, Akira Seto, Ichiro Matsunari, Yoshie Nakajima, Shintaro Nakano, Ichiei Kuji","doi":"10.17996/anc.23-00008","DOIUrl":null,"url":null,"abstract":"<p><p><i>Background</i>: While the non-invasive assessment of cardiac sympathetic nerve dysfunction is readily accessible, its applicability in invasive intervention for structural heart disease has received limited investigation. Our study aimed to clarify the cardiac sympathetic nerve function in patients with severe Aortic stenosis (AS) and its postoperative changes after transcatheter aortic valve implantation (TAVI) using <sup>123</sup>I-metaiodobenzylguanidine scintigraphy (MIBG) in combination with 5-year mortality prediction model. <i>Methods</i>: Consecutive 26 patients (83±5ys, male 4) with severe AS who underwent MIBG prior TAVI procedures were retrospectively enrolled. Of those, 15 patients underwent postoperative-follow up MIBG. The early and delayed heart-to-mediastinum ratio (e- and d-H/M), and washout rate (WR) were obtained from MIBG planner imaging. The MIBG 5-year mortality prediction model was employed to compare pre and after TAVI. Cardiac function and wall thickness were evaluated with transthoracic echocardiography. <i>Results</i>: Preoperative e-H/M, d-H/M, and WR were 2.4±0.5, 2.3±0.4, and 29±14% respectively, and WR showed significant correlation to left ventricular ejection fraction (LVEF) and brain natriuretic peptide (BNP) (r=-0.4 and 0.6; p=0.03, and 0.001 for LVEF and BNP, respectively). 102±28 days after TAVI, either H/M or WR did not show significant improvement among enrolled patients (2.5±0.3, 2.3±0.4, and 30±11% for e-, d-H/M, and WR for after TAVI), while the BNP level was significantly reduced (128±691 and 94±194 pg/dl, for pre vs. after, p=0.008). Five patients showed a significant recovery in WR (37.0±13.8 and 28.8±8.5% for pre and post, p=0.04), and left ventricular wall thickness was significantly thinner compared to those who did not recover (15.2±3.2 vs 11.2±2.4, p=0.02; 14.2±2.9 vs 10.8±1.8, p=0.02 for intraventricular septum and posterior wall, respectively). In 5-year prediction risk model, 7 patients showed a significant reduction in mortality risk, and the patients who did not show risk reduction had significantly reduced renal function (eGFR 57.5±18.8 vs. 38.2±11.3 ml/min/1.73m<sup>2</sup>, p=0.03 for recovered vs. not recovered). <i>Conclusion</i>: After a 3-month follow-up after TAVI, diverse response in cardiac MIBG parameters were observed among patients with severe AS, despite successful valve replacement. Cardiac MIBG serves as a non-invasive tool that can comprehensively evaluate and surrogate the severity of heart failure resulting from a multi-factorial condition.</p>","PeriodicalId":72228,"journal":{"name":"Annals of nuclear cardiology","volume":"10 1","pages":"6-15"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11612390/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of nuclear cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17996/anc.23-00008","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
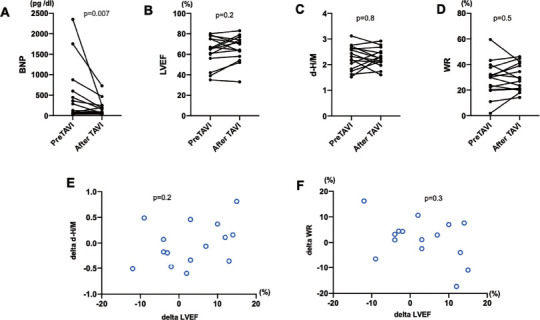
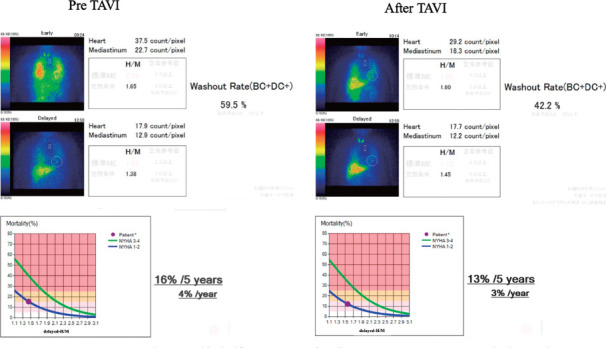
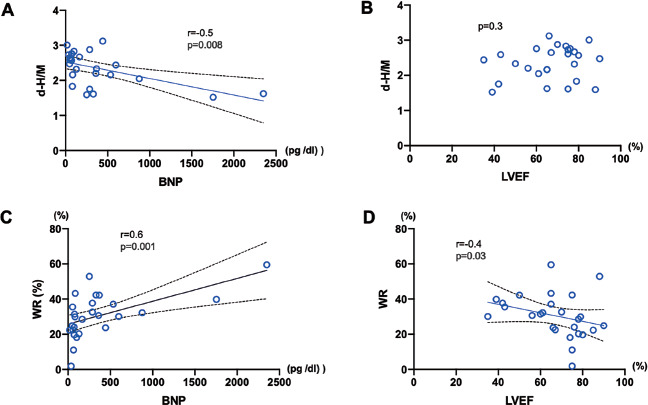
Background: While the non-invasive assessment of cardiac sympathetic nerve dysfunction is readily accessible, its applicability in invasive intervention for structural heart disease has received limited investigation. Our study aimed to clarify the cardiac sympathetic nerve function in patients with severe Aortic stenosis (AS) and its postoperative changes after transcatheter aortic valve implantation (TAVI) using 123I-metaiodobenzylguanidine scintigraphy (MIBG) in combination with 5-year mortality prediction model. Methods: Consecutive 26 patients (83±5ys, male 4) with severe AS who underwent MIBG prior TAVI procedures were retrospectively enrolled. Of those, 15 patients underwent postoperative-follow up MIBG. The early and delayed heart-to-mediastinum ratio (e- and d-H/M), and washout rate (WR) were obtained from MIBG planner imaging. The MIBG 5-year mortality prediction model was employed to compare pre and after TAVI. Cardiac function and wall thickness were evaluated with transthoracic echocardiography. Results: Preoperative e-H/M, d-H/M, and WR were 2.4±0.5, 2.3±0.4, and 29±14% respectively, and WR showed significant correlation to left ventricular ejection fraction (LVEF) and brain natriuretic peptide (BNP) (r=-0.4 and 0.6; p=0.03, and 0.001 for LVEF and BNP, respectively). 102±28 days after TAVI, either H/M or WR did not show significant improvement among enrolled patients (2.5±0.3, 2.3±0.4, and 30±11% for e-, d-H/M, and WR for after TAVI), while the BNP level was significantly reduced (128±691 and 94±194 pg/dl, for pre vs. after, p=0.008). Five patients showed a significant recovery in WR (37.0±13.8 and 28.8±8.5% for pre and post, p=0.04), and left ventricular wall thickness was significantly thinner compared to those who did not recover (15.2±3.2 vs 11.2±2.4, p=0.02; 14.2±2.9 vs 10.8±1.8, p=0.02 for intraventricular septum and posterior wall, respectively). In 5-year prediction risk model, 7 patients showed a significant reduction in mortality risk, and the patients who did not show risk reduction had significantly reduced renal function (eGFR 57.5±18.8 vs. 38.2±11.3 ml/min/1.73m2, p=0.03 for recovered vs. not recovered). Conclusion: After a 3-month follow-up after TAVI, diverse response in cardiac MIBG parameters were observed among patients with severe AS, despite successful valve replacement. Cardiac MIBG serves as a non-invasive tool that can comprehensively evaluate and surrogate the severity of heart failure resulting from a multi-factorial condition.
背景:虽然心脏交感神经功能障碍的无创评估很容易获得,但其在结构性心脏病的有创干预中的适用性研究有限。本研究旨在利用123I-metaiodobenzylguanidine scintigraphy (MIBG)结合5年死亡率预测模型,明确重度主动脉瓣狭窄(AS)患者的心脏交感神经功能及其经导管主动脉瓣植入术(TAVI)后的变化。方法:回顾性研究连续26例(83±5岁,男性4例)重度AS患者在TAVI手术前行MIBG。其中,15例患者接受了术后随访MIBG。早期和延迟的心脏与纵隔比值(e-和d-H/M)和冲洗率(WR)通过MIBG计划器成像获得。采用MIBG 5年死亡率预测模型对TAVI前后进行比较。经胸超声心动图评价心功能和壁厚。结果:术前e-H/M、d-H/M、WR分别为2.4±0.5、2.3±0.4、29±14%,WR与左室射血分数(LVEF)、脑利钠肽(BNP)有显著相关性(r=-0.4、0.6;LVEF和BNP分别为p=0.03和0.001)。TAVI后102±28天,入组患者的H/M或WR均无显著改善(TAVI后e-、d-H/M和WR分别为2.5±0.3、2.3±0.4和30±11%),而BNP水平显著降低(术前和术后分别为128±691和94±194 pg/dl, p=0.008)。5例患者WR显著恢复(术前和术后分别为37.0±13.8和28.8±8.5%,p=0.04),左室壁厚度较未恢复者显著变薄(15.2±3.2 vs 11.2±2.4,p=0.02;脑室间隔和后壁分别为14.2±2.9 vs 10.8±1.8,p=0.02)。在5年预测风险模型中,7例患者死亡风险显著降低,未显示风险降低的患者肾功能显著降低(eGFR 57.5±18.8 vs 38.2±11.3 ml/min/1.73m2,康复vs未康复p=0.03)。结论:经过TAVI术后3个月的随访,尽管瓣膜置换术成功,但严重AS患者的心脏MIBG参数有不同的反应。心脏MIBG作为一种非侵入性工具,可以全面评估和替代多因素导致的心力衰竭的严重程度。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


