{"title":"Prognostic Impact of Therapeutic Agents for Septic-Associated Disseminated Intravascular Coagulation According to Different Sources of Infection.","authors":"Makoto Kobayashi, Kyohei Sakurai, Yoshimatsu Ehama","doi":"10.2147/OAEM.S484602","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Sepsis can be caused by various infectious sources; however, treatment strategies for secondary disseminated intravascular coagulation (DIC) differ between countries. The Japanese sepsis guidelines recommend the use of two drugs for DIC but do not specify which drugs should be used and under which conditions. No clear reports have compared the outcomes of DIC treatments based on the source of infection. This is the first study to clarify the difference in prognosis by the source of infection and compare the effect of the treatment of choice for DIC on prognosis.</p><p><strong>Patients and methods: </strong>This single-center, retrospective, nonrandomized cohort study included 411 patients with a confirmed diagnosis of sepsis-associated DIC who were initiated on DIC therapies. Recombinant thrombomodulin (rTM) preparation and antithrombin (AT) replacement therapy were the DIC therapies used. The patients were divided into five groups determined to be the primary source of infection for treatment: intestine-related, biliary tract, respiratory tract, urinary tract, and catheter-related bloodstream infections (CRBSIs). In addition to differences in DIC treatment, we evaluated the following three covariates that may influence mortality, considering the influence of background interactions at the infection source: serum albumin concentration, APACHE-II score, and blood antithrombin activity. A Cox proportional hazards model was used to assess the association between the covariates and compare their effect on 60-day survival.</p><p><strong>Results: </strong>Univariate analysis of the DIC drug choice results showed that survival was statistically significantly higher in the rTM arm for biliary tract infections (P = 0.002) and CRBSI (P = 0.021). However, multivariate analysis with other covariates showed that AT replacement therapy was statistically effective for respiratory tract infections (hazard ratio, 0.353; P = 0.027).</p><p><strong>Conclusion: </strong>Our study showed that the pathogenesis of severe sepsis with DIC differs depending on the source of infection which should be considered when developing treatment strategies. Particularly, the importance of anti-DIC drug selectivity based on the source of infection was confirmed.</p>","PeriodicalId":45096,"journal":{"name":"Open Access Emergency Medicine","volume":"16 ","pages":"285-295"},"PeriodicalIF":1.5000,"publicationDate":"2024-11-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11611707/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Access Emergency Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/OAEM.S484602","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Sepsis can be caused by various infectious sources; however, treatment strategies for secondary disseminated intravascular coagulation (DIC) differ between countries. The Japanese sepsis guidelines recommend the use of two drugs for DIC but do not specify which drugs should be used and under which conditions. No clear reports have compared the outcomes of DIC treatments based on the source of infection. This is the first study to clarify the difference in prognosis by the source of infection and compare the effect of the treatment of choice for DIC on prognosis.
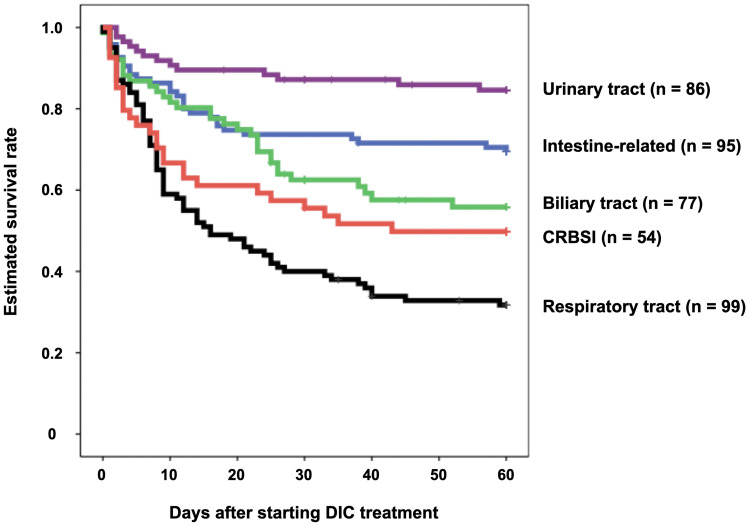
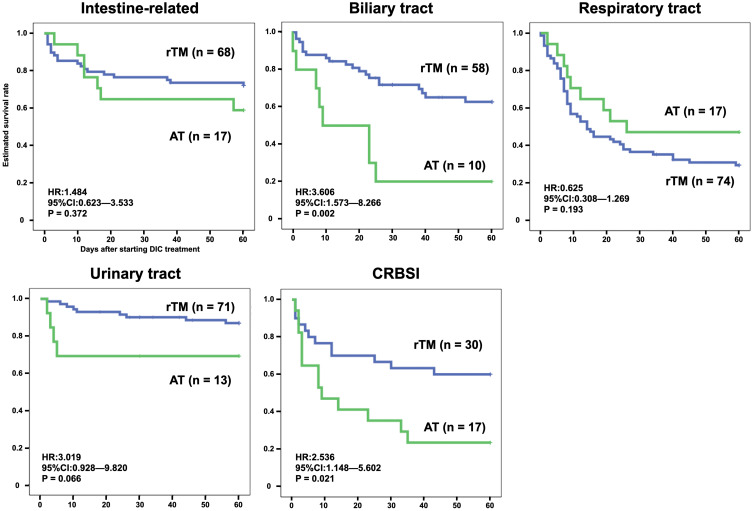
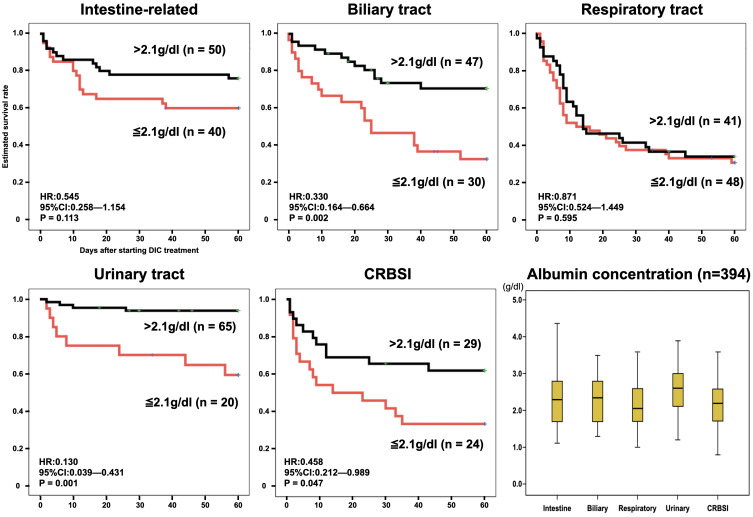
Patients and methods: This single-center, retrospective, nonrandomized cohort study included 411 patients with a confirmed diagnosis of sepsis-associated DIC who were initiated on DIC therapies. Recombinant thrombomodulin (rTM) preparation and antithrombin (AT) replacement therapy were the DIC therapies used. The patients were divided into five groups determined to be the primary source of infection for treatment: intestine-related, biliary tract, respiratory tract, urinary tract, and catheter-related bloodstream infections (CRBSIs). In addition to differences in DIC treatment, we evaluated the following three covariates that may influence mortality, considering the influence of background interactions at the infection source: serum albumin concentration, APACHE-II score, and blood antithrombin activity. A Cox proportional hazards model was used to assess the association between the covariates and compare their effect on 60-day survival.
Results: Univariate analysis of the DIC drug choice results showed that survival was statistically significantly higher in the rTM arm for biliary tract infections (P = 0.002) and CRBSI (P = 0.021). However, multivariate analysis with other covariates showed that AT replacement therapy was statistically effective for respiratory tract infections (hazard ratio, 0.353; P = 0.027).
Conclusion: Our study showed that the pathogenesis of severe sepsis with DIC differs depending on the source of infection which should be considered when developing treatment strategies. Particularly, the importance of anti-DIC drug selectivity based on the source of infection was confirmed.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


