{"title":"Feasibility and Safety of the C1 \"Zero Angle\" Screw: A Novel \"In-Out-In\" Technique for Atlantoaxial Dislocation.","authors":"Zexing Chen, Xinzhao Huang, Xiaobao Zou, Peirong Lian, Guoqiang Liu, Junlin Chen, Changrong Zhu, Xiangyang Ma","doi":"10.1111/os.14309","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To minimize the risk of V3 segment of vertebral artery (VA) injury in the atlantoaxial dislocation (AAD) patients with C1 pedicle height less than 4.0 mm and provide a strong toggle force in irreducible AAD and revision surgery. We evaluated the feasibility of C1 \"Zero Angle\" screw (C1ZAS) and safe entry point with \"in-out-in\" technique as an alternative option for C1 pedicle screw (PS) in cases with AAD.</p><p><strong>Methods: </strong>Sixty-one patients with AAD or atlantoaxial instability (AAI) (45 male and 16 female) who underwent cervical computed tomography and magnetic resonance imaging scans in our center between January 1, 2022 and December 31, 2023 were retrospectively reviewed. Measurements were made around the ideal trajectory and entry point of C1ZAS using computerized tomography (CT) and magnetic resonance imaging (MRI) in 61 patients. Radiographic measurements included (A) the distance from the recess to the transverse foramen (RTF); (B) the tricortical screw zone (TSZ); (C) the lateral mass height along the C1ZAS trajectory (LMH); (D) the screw length of C1ZAS (ZSL); (E) the screw length of C1 PS (PSL); (F) the distances from the recess to the dura (RD); (G) the distance from the recess to the spinal cord (RSC); (H) the distance from the inner of lateral mass to the spinal cord (ILMSC). During the period of January 1, 2022 to December 31, 2023, C1ZAS placement with \"in-out-in\" technique was used as an alternative option for C1 PS in 8 patients with AAD and unilateral/bilateral narrow C1 pedicles.</p><p><strong>Results: </strong>The average RTF, TSZ, LMH, ZSL, RD, RSC, and ILMSC were 7.71, 6.14, 8.32, 33.23, 4.68, 10.02, and 2.91 mm respectively. The entry point of the C1ZAS was defined as the projection point of the inner of the recess to the posterior arch and the trajectory should be angled cephalad by 8.7° and medially by 0°. The 61 patients (122 sides) with AAD or AAI were classified into three groups: the low-risk (76 sides, 62%), the intermedial-risk (18 sides, 15%), and the high-risk (28 sides, 23%) groups. Satisfactory C1ZAS placement and atlantoaxial reduction were achieved in all eight patients with AAD and unilateral/bilateral narrow C1 pedicles. No instance of C1ZAS placement-related VA injury or dural laceration was observed.</p><p><strong>Conclusions: </strong>When the placement of C1 PS is not feasible in patients with AAD and unilateral/bilateral narrow C1 pedicles, C1ZAS placement with \"in-out-in\" technique can be considered an effective alternative option, providing tricortical or quadricortical purchase for rigid fixation of the atlas.</p>","PeriodicalId":19566,"journal":{"name":"Orthopaedic Surgery","volume":" ","pages":"437-445"},"PeriodicalIF":2.1000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11787991/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Orthopaedic Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/os.14309","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To minimize the risk of V3 segment of vertebral artery (VA) injury in the atlantoaxial dislocation (AAD) patients with C1 pedicle height less than 4.0 mm and provide a strong toggle force in irreducible AAD and revision surgery. We evaluated the feasibility of C1 "Zero Angle" screw (C1ZAS) and safe entry point with "in-out-in" technique as an alternative option for C1 pedicle screw (PS) in cases with AAD.
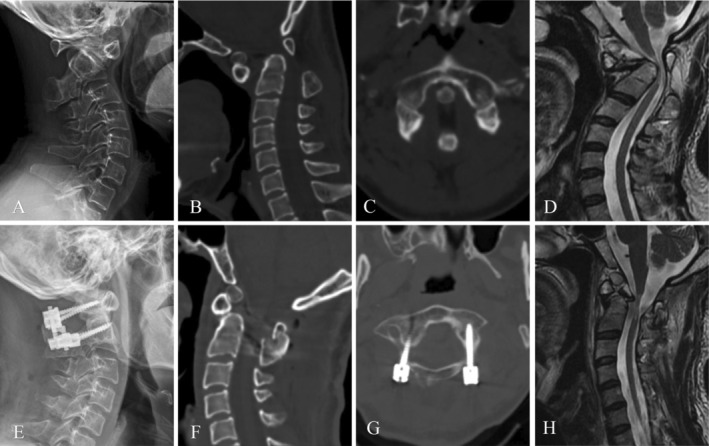
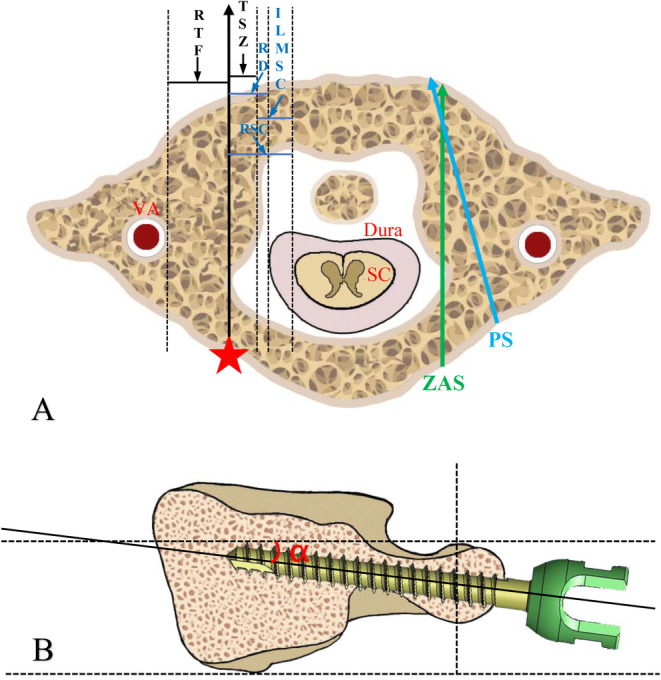
Methods: Sixty-one patients with AAD or atlantoaxial instability (AAI) (45 male and 16 female) who underwent cervical computed tomography and magnetic resonance imaging scans in our center between January 1, 2022 and December 31, 2023 were retrospectively reviewed. Measurements were made around the ideal trajectory and entry point of C1ZAS using computerized tomography (CT) and magnetic resonance imaging (MRI) in 61 patients. Radiographic measurements included (A) the distance from the recess to the transverse foramen (RTF); (B) the tricortical screw zone (TSZ); (C) the lateral mass height along the C1ZAS trajectory (LMH); (D) the screw length of C1ZAS (ZSL); (E) the screw length of C1 PS (PSL); (F) the distances from the recess to the dura (RD); (G) the distance from the recess to the spinal cord (RSC); (H) the distance from the inner of lateral mass to the spinal cord (ILMSC). During the period of January 1, 2022 to December 31, 2023, C1ZAS placement with "in-out-in" technique was used as an alternative option for C1 PS in 8 patients with AAD and unilateral/bilateral narrow C1 pedicles.
Results: The average RTF, TSZ, LMH, ZSL, RD, RSC, and ILMSC were 7.71, 6.14, 8.32, 33.23, 4.68, 10.02, and 2.91 mm respectively. The entry point of the C1ZAS was defined as the projection point of the inner of the recess to the posterior arch and the trajectory should be angled cephalad by 8.7° and medially by 0°. The 61 patients (122 sides) with AAD or AAI were classified into three groups: the low-risk (76 sides, 62%), the intermedial-risk (18 sides, 15%), and the high-risk (28 sides, 23%) groups. Satisfactory C1ZAS placement and atlantoaxial reduction were achieved in all eight patients with AAD and unilateral/bilateral narrow C1 pedicles. No instance of C1ZAS placement-related VA injury or dural laceration was observed.
Conclusions: When the placement of C1 PS is not feasible in patients with AAD and unilateral/bilateral narrow C1 pedicles, C1ZAS placement with "in-out-in" technique can be considered an effective alternative option, providing tricortical or quadricortical purchase for rigid fixation of the atlas.
期刊介绍:
Orthopaedic Surgery (OS) is the official journal of the Chinese Orthopaedic Association, focusing on all aspects of orthopaedic technique and surgery.
The journal publishes peer-reviewed articles in the following categories: Original Articles, Clinical Articles, Review Articles, Guidelines, Editorials, Commentaries, Surgical Techniques, Case Reports and Meeting Reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


