Allison M. Bock, Kerstin Wenzl, Joseph P. Novak, Matthew E. Stokes, Melissa A. Hopper, Jordan E. Krull, Abigail R. Dropik, Vivek Sarangi, Maria Ortiz, Nicholas Stong, C. Chris Huang, Matthew J. Maurer, Rebecca L. King, Umar Farooq, Yucai Wang, Thomas E. Witzig, Stephen M. Ansell, Thomas M. Habermann, James R. Cerhan, Anita K. Gandhi, Grzegorz Nowakowski, Anne J. Novak
{"title":"Molecular Features of Diffuse Large B-Cell Lymphoma Associated With Primary Treatment Resistance","authors":"Allison M. Bock, Kerstin Wenzl, Joseph P. Novak, Matthew E. Stokes, Melissa A. Hopper, Jordan E. Krull, Abigail R. Dropik, Vivek Sarangi, Maria Ortiz, Nicholas Stong, C. Chris Huang, Matthew J. Maurer, Rebecca L. King, Umar Farooq, Yucai Wang, Thomas E. Witzig, Stephen M. Ansell, Thomas M. Habermann, James R. Cerhan, Anita K. Gandhi, Grzegorz Nowakowski, Anne J. Novak","doi":"10.1002/hon.70006","DOIUrl":null,"url":null,"abstract":"<p>Diffuse large B-cell lymphoma (DLBCL) patients that fail to achieve a complete metabolic response with frontline immunochemotherapy have a poor prognosis. Genomic profiling has led to a broader understanding of the molecular drivers in DLBCL, but it is unknown how well current classifiers identify patients that will experience primary treatment resistance (PTR). Using whole exome and RNA sequencing data from newly diagnosed DLBCL patients, we evaluated the genomic landscape of PTR and compared it to that of non-PTR DLBCL. We found a significant increase in the frequency of <i>TP53</i> (34% vs. 15%, <i>p</i> = 0.005) and <i>ARID1A</i> mutations (21% vs. 7%, <i>p</i> = 0.007) in PTR cases, with pathway analysis further demonstrating a downregulation of TP53 and an increase in chromatin modifying pathways. These results suggest that <i>TP53</i> and <i>ARID1A</i> may be key mediators of PTR and important pathways contributing to the poor outcomes. We found that the current molecular classifiers were unable to identify PTR cases at diagnosis. However, our newly identified high-risk signature identified 46% of PTR cases at diagnosis. Overall, these results contribute to our understanding of the genomic landscape of patients with primary treatment resistance.</p>","PeriodicalId":12882,"journal":{"name":"Hematological Oncology","volume":"43 1","pages":""},"PeriodicalIF":3.3000,"publicationDate":"2024-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/hon.70006","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hematological Oncology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/hon.70006","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
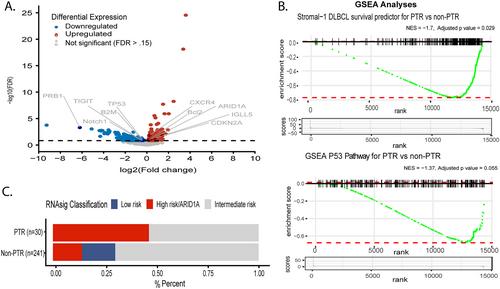
Diffuse large B-cell lymphoma (DLBCL) patients that fail to achieve a complete metabolic response with frontline immunochemotherapy have a poor prognosis. Genomic profiling has led to a broader understanding of the molecular drivers in DLBCL, but it is unknown how well current classifiers identify patients that will experience primary treatment resistance (PTR). Using whole exome and RNA sequencing data from newly diagnosed DLBCL patients, we evaluated the genomic landscape of PTR and compared it to that of non-PTR DLBCL. We found a significant increase in the frequency of TP53 (34% vs. 15%, p = 0.005) and ARID1A mutations (21% vs. 7%, p = 0.007) in PTR cases, with pathway analysis further demonstrating a downregulation of TP53 and an increase in chromatin modifying pathways. These results suggest that TP53 and ARID1A may be key mediators of PTR and important pathways contributing to the poor outcomes. We found that the current molecular classifiers were unable to identify PTR cases at diagnosis. However, our newly identified high-risk signature identified 46% of PTR cases at diagnosis. Overall, these results contribute to our understanding of the genomic landscape of patients with primary treatment resistance.
弥漫性大b细胞淋巴瘤(DLBCL)患者在一线免疫化疗中未能达到完全的代谢反应,预后较差。基因组分析使人们对DLBCL的分子驱动因素有了更广泛的了解,但目前尚不清楚目前的分类器在多大程度上识别出将经历原发性治疗耐药(PTR)的患者。利用新诊断的DLBCL患者的全外显子组和RNA测序数据,我们评估了PTR的基因组图谱,并将其与非PTR的DLBCL进行了比较。我们发现PTR病例中TP53 (34% vs. 15%, p = 0.005)和ARID1A突变(21% vs. 7%, p = 0.007)的频率显著增加,通路分析进一步表明TP53下调和染色质修饰通路增加。这些结果表明,TP53和ARID1A可能是PTR的关键介质和导致不良预后的重要途径。我们发现目前的分子分类器无法在诊断时识别PTR病例。然而,我们新发现的高风险特征在诊断时识别了46%的PTR病例。总的来说,这些结果有助于我们了解原发性治疗耐药患者的基因组景观。
期刊介绍:
Hematological Oncology considers for publication articles dealing with experimental and clinical aspects of neoplastic diseases of the hemopoietic and lymphoid systems and relevant related matters. Translational studies applying basic science to clinical issues are particularly welcomed. Manuscripts dealing with the following areas are encouraged:
-Clinical practice and management of hematological neoplasia, including: acute and chronic leukemias, malignant lymphomas, myeloproliferative disorders
-Diagnostic investigations, including imaging and laboratory assays
-Epidemiology, pathology and pathobiology of hematological neoplasia of hematological diseases
-Therapeutic issues including Phase 1, 2 or 3 trials as well as allogeneic and autologous stem cell transplantation studies
-Aspects of the cell biology, molecular biology, molecular genetics and cytogenetics of normal or diseased hematopoeisis and lymphopoiesis, including stem cells and cytokines and other regulatory systems.
Concise, topical review material is welcomed, especially if it makes new concepts and ideas accessible to a wider community. Proposals for review material may be discussed with the Editor-in-Chief. Collections of case material and case reports will be considered only if they have broader scientific or clinical relevance.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


