Isobel Masson Francis Todd, Maria Christine Magnus, Lars Henning Pedersen, David Burgner, Jessica Eden Miller
{"title":"Caesarean section and risk of infection in offspring: systematic review and meta-analysis of observational studies.","authors":"Isobel Masson Francis Todd, Maria Christine Magnus, Lars Henning Pedersen, David Burgner, Jessica Eden Miller","doi":"10.1136/bmjmed-2024-000995","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare the risk of hospital admissions with infections and infections not in hospital in children born by caesarean section with children born by vaginal birth.</p><p><strong>Data sources: </strong>Medline, Embase, and PubMed were searched with no restriction on start date up to 12 February 2024.</p><p><strong>Study selection: </strong>Observational studies were included that reported the association between caesarean section and vaginal birth in relation to the risk of infections (both those that lead to hospital admission and those that do not) up to 18 years of age. Studies were excluded if they were not representative of a general population or if they focused on congenital, neonatal, or vertically acquired infections. No restrictions were made for language, publication date, or setting.</p><p><strong>Review methods: </strong>Findings for hospital admissions with infection were synthesised by meta-analyses of specific infection outcomes and type of caesarean birth (emergency <i>v</i> elective) and findings for other infections (ie, infection episodes reported by parents and primary care visits) by direction of effect. Risk of bias was assessed using the ROBINS-E tool and the overall certainty of evidence through the GRADE framework.</p><p><strong>Results: </strong>31 eligible studies of over 10 million children were included. Findings were from population-based birth cohorts and registry data linkage studies in high income countries. Cohort sizes ranged from 288 to 7.2 million and follow up age was from one to 18 years. Outcomes included overall and specific clinical categories of infection. From studies of overall admission to hospital with infection, the proportion of children admitted ranged between 9-29% across exposure groups. In random-effects meta-analyses combining hazard ratios, children delivered by caesarean section had an increased rate of hospital admission with infections overall and in three common clinical infection categories: (1) overall admissions to hospital with infection (emergency caesarean section: n=6 study populations, hazard ratio 1.10 (95% confidence interval 1.06 to 1.14), <math><mi>τ</mi></math> <sup>2</sup>=0.0009, I<sup>2</sup>=96%; elective caesarean section: n=7, 1.12 (1.09 to 1.15), <math><mi>τ</mi></math> <sup>2</sup>=0.0006, I<sup>2</sup>=88%); (2) admission to hospital for upper respiratory infections (emergency caesarean section: n=7, 1.11 (1.09 to 1.13), <math><mi>τ</mi></math> <sup>2</sup>=0.0003, I<sup>2</sup>=73%; elective caesarean section: n=7, 1.16 (1.12 to 1.20), <math><mi>τ</mi></math> <sup>2</sup>=0.0012, I<sup>2</sup>=89%); (3) admission to hospital for lower respiratory infections (emergency caesarean section: n=8, 1.09 (1.06 to 1.12), <math><mi>τ</mi></math> <sup>2</sup>=0.0010, I<sup>2</sup>=88%; elective caesarean section: n=8, 1.13 (1.10 to 1.16), <math><mi>τ</mi></math> <sup>2</sup>=0.0009, I<sup>2</sup>=84%); (4) admission to hospital for gastrointestinal infections (emergency caesarean section: n=7, 1.19 (1.13 to 1.26), <math><mi>τ</mi></math> <sup>2</sup>=0.0025, I<sup>2</sup>=86%; elective caesarean section: n=7, 1.20 (1.15 to 1.25), <math><mi>τ</mi></math> <sup>2</sup>=0.0009, I<sup>2</sup>=67%). Eight of 11 studies of other infections suggested an increased risk of their primary infection outcome in those born by caesarean section. Risk of bias concerns primarily related to confounding.</p><p><strong>Conclusions: </strong>Findings from high income countries showed a consistent association between caesarean section birth and greater risk of infections in children across various settings. Limitations of existing studies include the potential for unmeasured confounding, specifically confounding by indication, and a scarcity of studies from low and middle income countries.</p><p><strong>Review registration: </strong>PROSPERO (CRD42022369252).</p>","PeriodicalId":72433,"journal":{"name":"BMJ medicine","volume":"3 1","pages":"e000995"},"PeriodicalIF":10.0000,"publicationDate":"2024-11-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11603743/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjmed-2024-000995","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To compare the risk of hospital admissions with infections and infections not in hospital in children born by caesarean section with children born by vaginal birth.
Data sources: Medline, Embase, and PubMed were searched with no restriction on start date up to 12 February 2024.
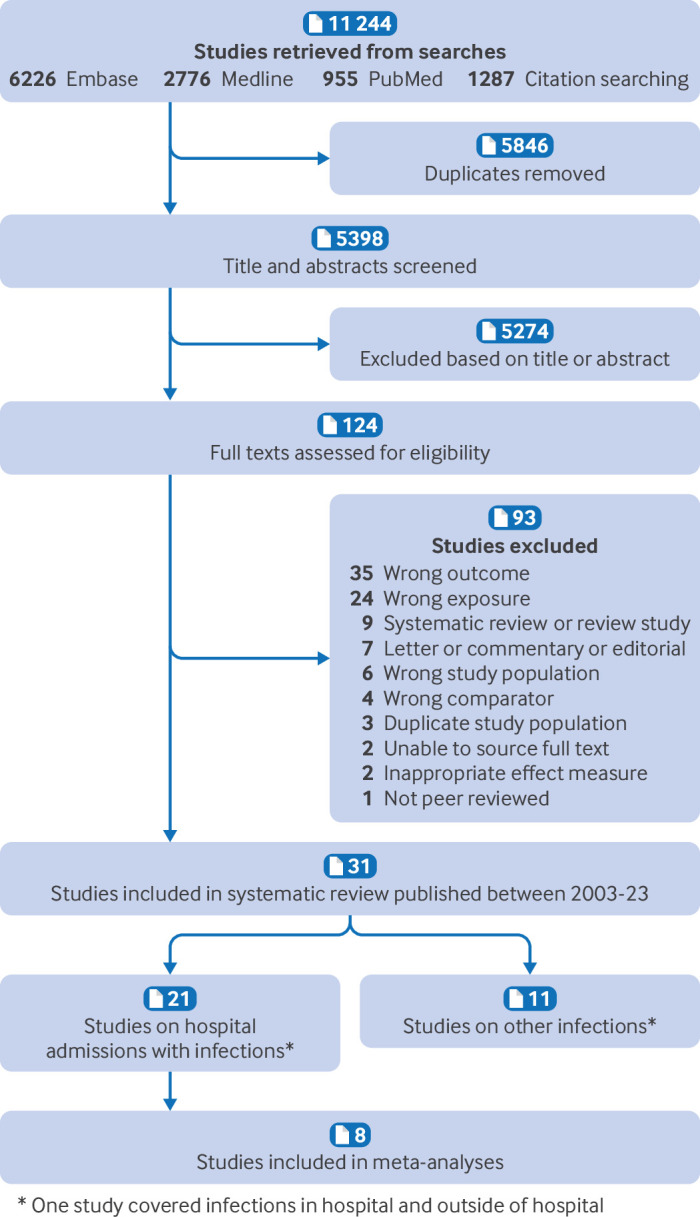
Study selection: Observational studies were included that reported the association between caesarean section and vaginal birth in relation to the risk of infections (both those that lead to hospital admission and those that do not) up to 18 years of age. Studies were excluded if they were not representative of a general population or if they focused on congenital, neonatal, or vertically acquired infections. No restrictions were made for language, publication date, or setting.
Review methods: Findings for hospital admissions with infection were synthesised by meta-analyses of specific infection outcomes and type of caesarean birth (emergency v elective) and findings for other infections (ie, infection episodes reported by parents and primary care visits) by direction of effect. Risk of bias was assessed using the ROBINS-E tool and the overall certainty of evidence through the GRADE framework.
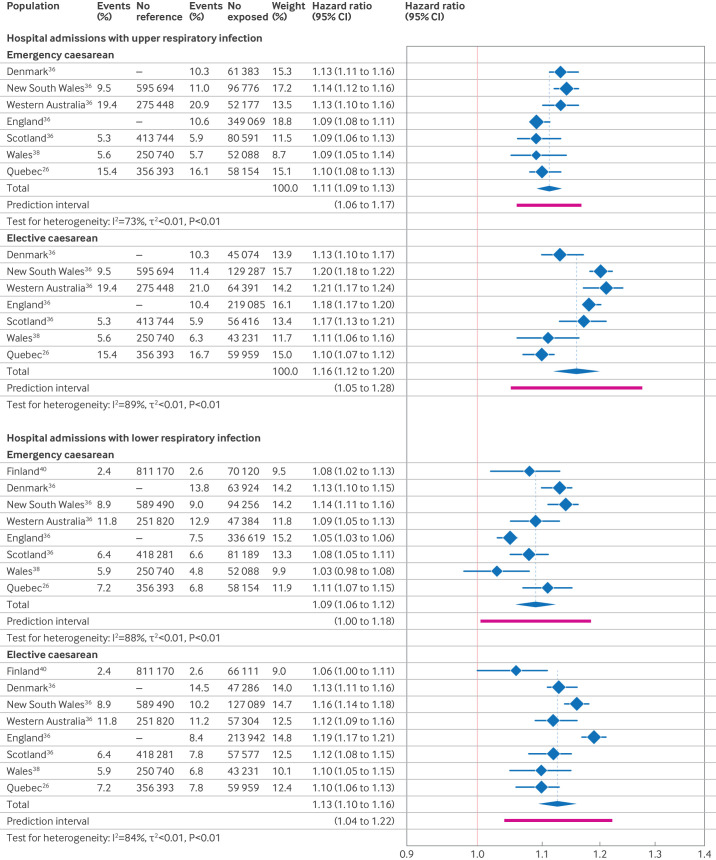
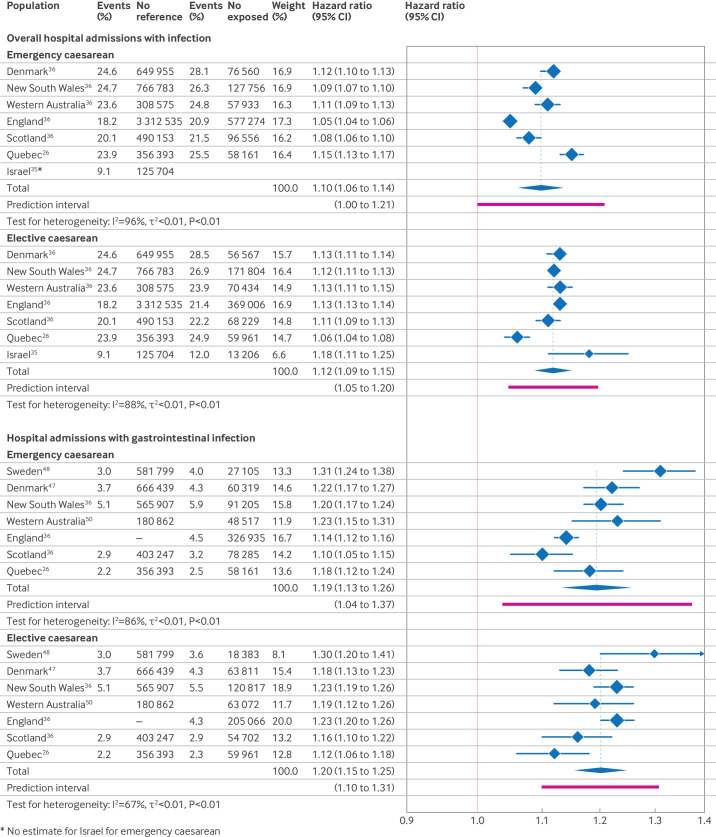
Results: 31 eligible studies of over 10 million children were included. Findings were from population-based birth cohorts and registry data linkage studies in high income countries. Cohort sizes ranged from 288 to 7.2 million and follow up age was from one to 18 years. Outcomes included overall and specific clinical categories of infection. From studies of overall admission to hospital with infection, the proportion of children admitted ranged between 9-29% across exposure groups. In random-effects meta-analyses combining hazard ratios, children delivered by caesarean section had an increased rate of hospital admission with infections overall and in three common clinical infection categories: (1) overall admissions to hospital with infection (emergency caesarean section: n=6 study populations, hazard ratio 1.10 (95% confidence interval 1.06 to 1.14), 2=0.0009, I2=96%; elective caesarean section: n=7, 1.12 (1.09 to 1.15), 2=0.0006, I2=88%); (2) admission to hospital for upper respiratory infections (emergency caesarean section: n=7, 1.11 (1.09 to 1.13), 2=0.0003, I2=73%; elective caesarean section: n=7, 1.16 (1.12 to 1.20), 2=0.0012, I2=89%); (3) admission to hospital for lower respiratory infections (emergency caesarean section: n=8, 1.09 (1.06 to 1.12), 2=0.0010, I2=88%; elective caesarean section: n=8, 1.13 (1.10 to 1.16), 2=0.0009, I2=84%); (4) admission to hospital for gastrointestinal infections (emergency caesarean section: n=7, 1.19 (1.13 to 1.26), 2=0.0025, I2=86%; elective caesarean section: n=7, 1.20 (1.15 to 1.25), 2=0.0009, I2=67%). Eight of 11 studies of other infections suggested an increased risk of their primary infection outcome in those born by caesarean section. Risk of bias concerns primarily related to confounding.
Conclusions: Findings from high income countries showed a consistent association between caesarean section birth and greater risk of infections in children across various settings. Limitations of existing studies include the potential for unmeasured confounding, specifically confounding by indication, and a scarcity of studies from low and middle income countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


