Objective: Monochorionic twin gestations affected by Type-II selective fetal growth restriction (sFGR) are at increased risk of intrauterine fetal demise, extreme preterm birth, severe neurodevelopmental impairment (NDI) and neonatal death of one or both twins. In the absence of a consensus on the optimal management strategy, we chose to evaluate which strategy was cost-effective in the setting of Type-II sFGR.
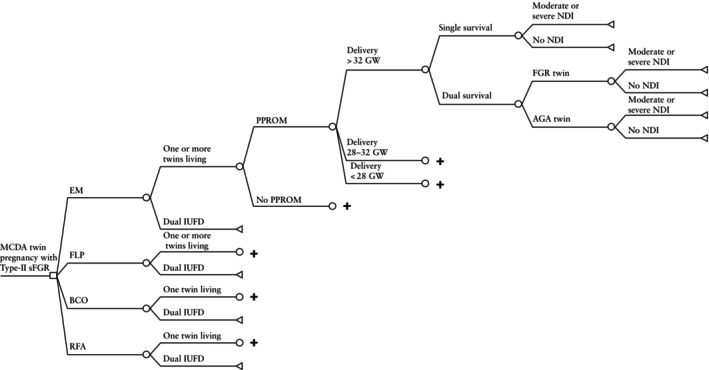
Methods: A decision-analytic model was used to compare expectant management (EM), bipolar cord occlusion (BCO), radiofrequency ablation (RFA) and fetoscopic laser photocoagulation (FLP) for a hypothetical cohort of 10 000 people with a monochorionic diamniotic twin pregnancy affected by Type-II sFGR. Probabilities and utilities were derived from the literature. Costs were derived from the Healthcare Cost and Utilization Project and adjusted to 2023 USD. The analytic horizon, taken from the perspective of the pregnant patient, extended throughout the life of the child or children. An incremental cost-effectiveness ratio of 50 000 USD per quality-adjusted life year defined the willingness-to-pay threshold. One-way and probabilistic sensitivity analysis was also performed.
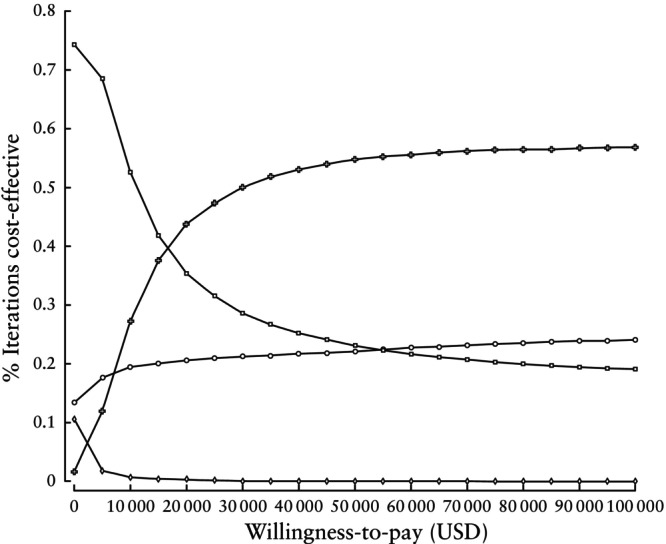
Results: For base-case estimates, RFA was the most cost-effective strategy compared with all of the other interventions included, with an incremental cost-effectiveness ratio of 14 243 USD per quality-adjusted life year. One-way sensitivity analysis demonstrated that the utilities assigned to fetal demise and severe NDI, as well as the costs of preterm birth before 32 weeks, most strongly impacted the model outcomes. On probabilistic sensitivity analysis, RFA was the most cost-effective strategy in 78% of runs, followed by BCO at 20%, EM at 2% and FLP in 0% of runs. When compared with EM, RFA led to 58 fewer births before 28 weeks' gestation, 273 fewer cases of severe NDI and 22 more deliveries after 32 weeks. When compared with FLP, RFA resulted in 259 fewer cases of severe NDI and 3177 more births after 32 weeks. When compared with BCO, RFA resulted in 1786 more neurologically intact neonates and 34 fewer cases of severe NDI.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


