Objectives: First, to compare the predictive performance of routine ultrasonographic estimated fetal weight (EFW) at 31 + 0 to 33 + 6 and 35 + 0 to 36 + 6 weeks' gestation for delivery of a small-for-gestational-age (SGA) neonate. Second, to compare the predictive performance of EFW at 36 weeks' gestation for SGA vs fetal growth restriction (FGR) at birth. Third, to compare the predictive performance for delivery of a SGA neonate of EFW < 10th percentile vs a model combining maternal demographic characteristics and elements of medical history with EFW.
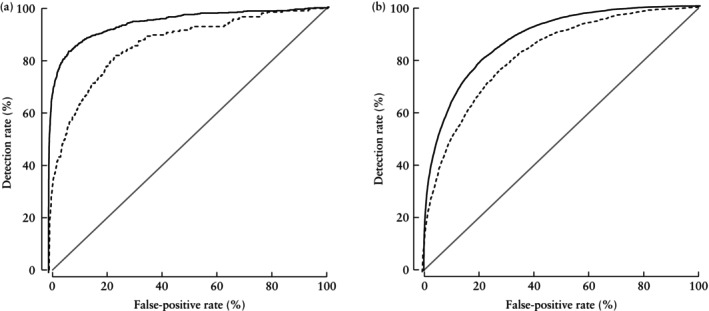
Methods: This was a retrospective analysis of prospectively collected data in 21 676 women with a singleton pregnancy who had undergone routine ultrasound examination at 31 + 0 to 33 + 6 weeks' gestation and 107 875 women with a singleton pregnancy who had undergone routine ultrasound examination at 35 + 0 to 36 + 6 weeks. Measurements of fetal head circumference, abdominal circumference and femur length were used to calculate EFW according to the Hadlock formula and this was expressed as a percentile according to the Fetal Medicine Foundation fetal and neonatal population weight charts. The same charts were used to diagnose SGA neonates with birth weight < 10th or < 3rd percentile. FGR was defined as birth weight < 10th percentile in addition to Doppler anomalies. For each gestational-age window at screening, the screen-positive rate and detection rate were calculated at different EFW cut-offs between the 10th and 50th percentiles for predicting the delivery of a SGA neonate with birth weight < 10th or < 3rd percentile, either within 2 weeks or at any time after assessment. The areas under the receiver-operating-characteristics curves (AUC) of screening for a SGA neonate by EFW at 31 + 0 to 33 + 6 weeks and at 35 + 0 to 36 + 6 weeks were compared.
Results: The predictive performance of routine ultrasonographic examination during the third trimester for delivery of a SGA neonate is higher if: first, the scan is carried out at 35 + 0 to 36 + 6 weeks' gestation rather than at 31 + 0 to 33 + 6 weeks; second, the outcome measure is birth weight < 3rd rather than < 10th percentile; third, the outcome measure is FGR rather than SGA; fourth, if delivery occurs within 2 weeks after assessment rather than at any time after assessment; and fifth, prediction is performed using a model that combines maternal demographic characteristics and elements of medical history with EFW rather than EFW < 10th percentile alone. At 35 + 0 to 36 + 6 weeks' gestation, detection of ≥ 85% of SGA neonates with birth weight < 10th percentile born at any time after assessment necessitates the use of EFW < 40th percentile. Screening at this percentile cut-off predicted 95% and 98% of neonates with birth weight < 10th and < 3rd percentile, respectively, born within 2 weeks after assessment, and the respective values for neonates born at any time after assessment were 85% and 93%.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


