Perinatal outcomes after selective third-trimester ultrasound screening for small-for-gestational age: prospective cohort study nested within DESiGN randomized controlled trial.
C Winsloe, J Elhindi, M C Vieira, S Relph, C G Arcus, K Coxon, A Briley, M Johnson, L M Page, A Shennan, N Marlow, C Lees, D A Lawlor, A Khalil, J Sandall, A Copas, D Pasupathy
Objective: In screening for small-for-gestational age (SGA) using third-trimester antenatal ultrasound, there are concerns about the low detection rates and potential for harm caused by both false-negative and false-positive screening results. Using a selective third-trimester ultrasound screening program, this study aimed to investigate the incidence of adverse perinatal outcomes among cases with (i) false-negative compared with true-positive SGA diagnosis and (ii) false-positive compared with true-negative SGA diagnosis.
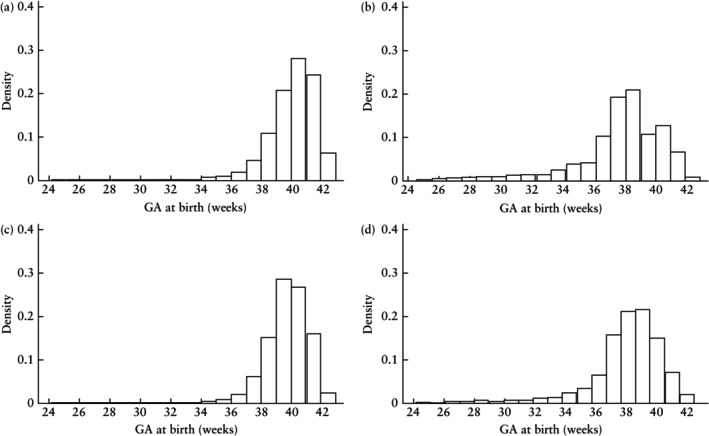
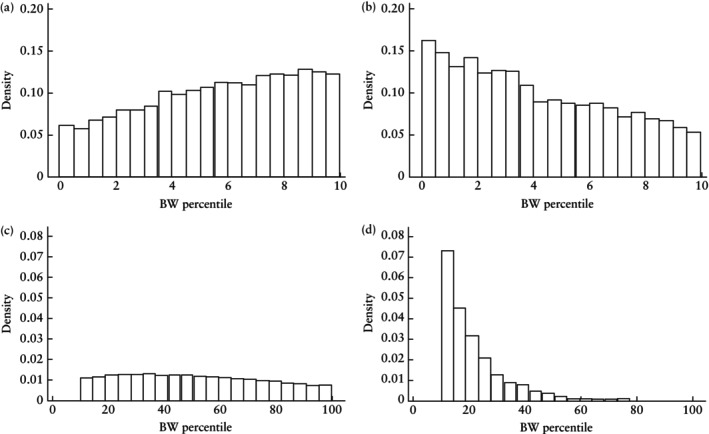
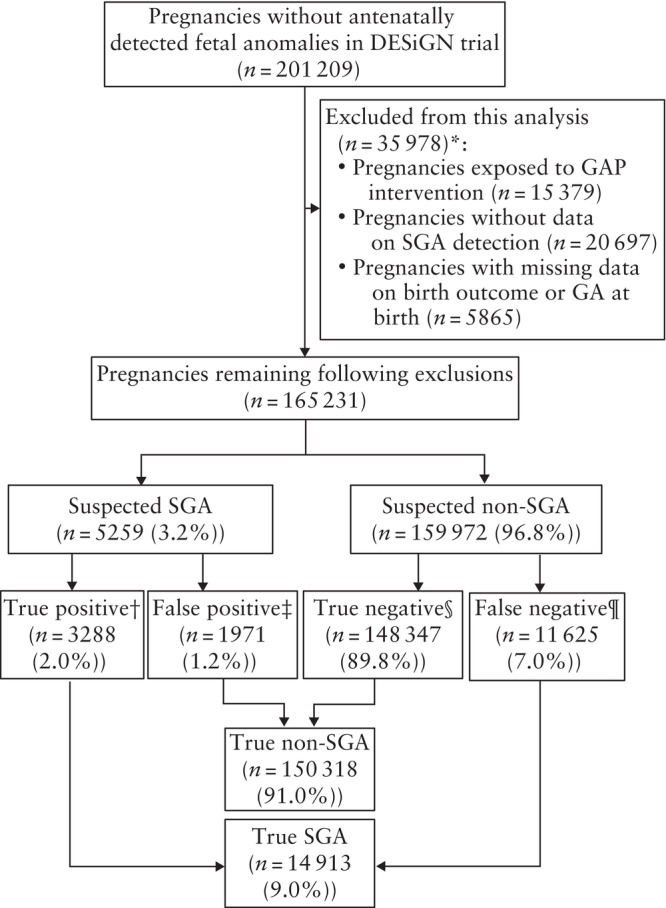
Methods: This prospective cohort study was nested within the UK-based DESiGN trial, a prospective multicenter cohort study of singleton pregnancies without antenatally detected fetal anomalies, born at > 24 + 0 to < 43 + 0 weeks' gestation. We included women recruited to the baseline period, or control arm, of the trial who were not exposed to the Growth Assessment Protocol intervention and whose birth outcomes were known. Stillbirth and major neonatal morbidity were the two primary outcomes. Minor neonatal morbidity was considered a secondary outcome. Suspected SGA was defined as an estimated fetal weight (EFW) < 10th percentile, based on the Hadlock formula and fetal growth charts. Similarly, SGA at birth was defined as birth weight (BW) < 10th percentile, based on UK population references. Maternal and pregnancy characteristics and perinatal outcomes were reported according to whether SGA was suspected antenatally or not. Unadjusted and adjusted logistic regression models were used to quantify the differences in adverse perinatal outcomes between the screening results (false negative vs true positive and false positive vs true negative).
Results: In total, 165 321 pregnancies were included in the analysis. Fetuses with a false-negative SGA screening result, compared to those with a true-positive result, were at a significantly higher risk of stillbirth (adjusted odds ratio (aOR), 1.18 (95% CI, 1.07-1.31)), but at lower risk of major (aOR, 0.87 (95% CI, 0.83-0.91)) and minor (aOR, 0.56, (95% CI, 0.54-0.59)) neonatal morbidity. Compared with a true-negative screening result, a false-positive result was associated with a lower BW percentile (median, 18.1 (interquartile range (IQR), 13.3-26.9) vs 49.9 (IQR, 30.3-71.7)). A false-positive result was also associated with a significantly increased risk of stillbirth (aOR, 2.24 (95% CI, 1.88-2.68)) and minor neonatal morbidity (aOR, 1.60 (95% CI, 1.51-1.71)), but not major neonatal morbidity (aOR, 1.04 (95% CI, 0.98-1.09)).
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


