Osama Hallak, Karley Fischer, Shaina Ailawadi, Damian Valencia, Yan Yatsynovich, Raja Nazir, Brian Schwartz
{"title":"Effects of Bioprosthetic Valve Fracturing on Valve-in-Valve Transcatheter Aortic Valve Implantation Transvalvular Gradients.","authors":"Osama Hallak, Karley Fischer, Shaina Ailawadi, Damian Valencia, Yan Yatsynovich, Raja Nazir, Brian Schwartz","doi":"10.14503/THIJ-23-8304","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is quickly becoming a routine and effective means by which to treat degenerated bioprosthetic valves. A known complication of ViV-TAVI is patient-prosthesis mismatch, which substantially affects survival. Bioprosthetic valve fracture is a method by which to reduce the risk of patient-prosthesis mismatch and post-ViV-TAVI transvalvular gradients. This study sought to determine the safety and efficacy of post-ViV-TAVI bioprosthetic valve fracture.</p><p><strong>Methods: </strong>Patients with a history of surgical aortic valve replacement undergoing ViV-TAVI bioprosthetic valve fracture (N = 25) at the corresponding institution from 2015 to 2022 were cataloged for a retrospective analysis. The implanted transcatheter valves were Medtronic Evolut R, Evolut PRO, and Evolut PRO+. Gradients were assessed before and after implantation and after fracturing using transthoracic echocardiogram.</p><p><strong>Results: </strong>The mean left ventricular ejection fraction of patients who underwent fracturing was 55.04%. The average (SD) peak and mean (SD) transvalvular gradients before the intervention were 68.17 (19.09) mm Hg and 38.98 (14.37) mm Hg, respectively. After ViV-TAVI, the same gradients were reduced to 27.25 (12.27) mm Hg and 15.63 (6.47) mm Hg, respectively. After bioprosthetic valve fracture, the gradients further decreased to 17.59 (7.93) mm Hg and 8.860 (3.334) mm Hg, respectively. The average reduction in peak gradient associated with fracturing was 12.07 mm Hg (95% CI, 5.73-18.41 mm Hg; <i>P</i> = .001). The average reduction in mean gradient associated with valve fracturing was 6.97 mm Hg (95% CI, 3.99-9.74 mm Hg; <i>P</i> < .001).</p><p><strong>Conclusion: </strong>Bioprosthetic valve fracture is a viable option for reducing residual transvalvular gradients after ViV-TAVI and should be considered in patients with elevated gradients (>20 mm Hg) or with concern for patient-prosthesis mismatch in patients who have an unacceptable risk for a redo sternotomy and surgical aortic valve replacement.</p>","PeriodicalId":48680,"journal":{"name":"Texas Heart Institute Journal","volume":"51 2","pages":"e238304"},"PeriodicalIF":0.9000,"publicationDate":"2024-11-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11584884/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Texas Heart Institute Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14503/THIJ-23-8304","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) is quickly becoming a routine and effective means by which to treat degenerated bioprosthetic valves. A known complication of ViV-TAVI is patient-prosthesis mismatch, which substantially affects survival. Bioprosthetic valve fracture is a method by which to reduce the risk of patient-prosthesis mismatch and post-ViV-TAVI transvalvular gradients. This study sought to determine the safety and efficacy of post-ViV-TAVI bioprosthetic valve fracture.
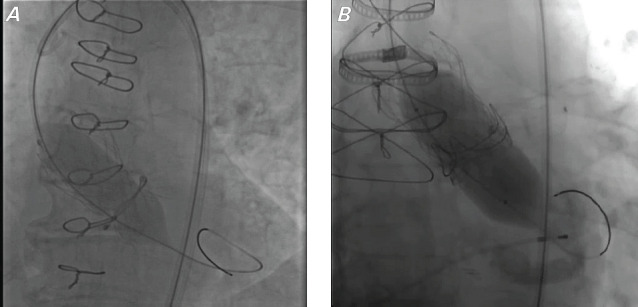
Methods: Patients with a history of surgical aortic valve replacement undergoing ViV-TAVI bioprosthetic valve fracture (N = 25) at the corresponding institution from 2015 to 2022 were cataloged for a retrospective analysis. The implanted transcatheter valves were Medtronic Evolut R, Evolut PRO, and Evolut PRO+. Gradients were assessed before and after implantation and after fracturing using transthoracic echocardiogram.
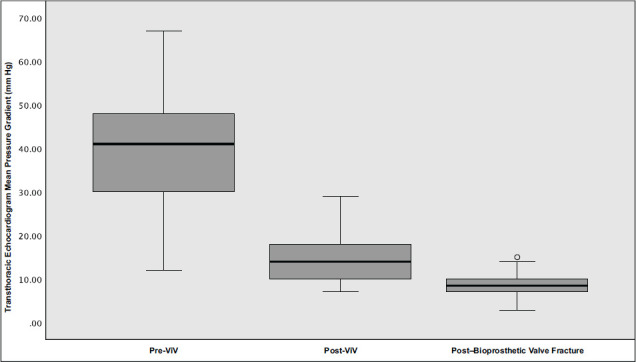
Results: The mean left ventricular ejection fraction of patients who underwent fracturing was 55.04%. The average (SD) peak and mean (SD) transvalvular gradients before the intervention were 68.17 (19.09) mm Hg and 38.98 (14.37) mm Hg, respectively. After ViV-TAVI, the same gradients were reduced to 27.25 (12.27) mm Hg and 15.63 (6.47) mm Hg, respectively. After bioprosthetic valve fracture, the gradients further decreased to 17.59 (7.93) mm Hg and 8.860 (3.334) mm Hg, respectively. The average reduction in peak gradient associated with fracturing was 12.07 mm Hg (95% CI, 5.73-18.41 mm Hg; P = .001). The average reduction in mean gradient associated with valve fracturing was 6.97 mm Hg (95% CI, 3.99-9.74 mm Hg; P < .001).
Conclusion: Bioprosthetic valve fracture is a viable option for reducing residual transvalvular gradients after ViV-TAVI and should be considered in patients with elevated gradients (>20 mm Hg) or with concern for patient-prosthesis mismatch in patients who have an unacceptable risk for a redo sternotomy and surgical aortic valve replacement.
期刊介绍:
For more than 45 years, the Texas Heart Institute Journal has been published by the Texas Heart Institute as part of its medical education program. Our bimonthly peer-reviewed journal enjoys a global audience of physicians, scientists, and healthcare professionals who are contributing to the prevention, diagnosis, and treatment of cardiovascular disease.
The Journal was printed under the name of Cardiovascular Diseases from 1974 through 1981 (ISSN 0093-3546). The name was changed to Texas Heart Institute Journal in 1982 and was printed through 2013 (ISSN 0730-2347). In 2014, the Journal moved to online-only publication. It is indexed by Index Medicus/MEDLINE and by other indexing and abstracting services worldwide. Our full archive is available at PubMed Central.
The Journal invites authors to submit these article types for review:
-Clinical Investigations-
Laboratory Investigations-
Reviews-
Techniques-
Coronary Anomalies-
History of Medicine-
Case Reports/Case Series (Submission Fee: $70.00 USD)-
Images in Cardiovascular Medicine (Submission Fee: $35.00 USD)-
Guest Editorials-
Peabody’s Corner-
Letters to the Editor

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


