{"title":"A New \"Tube-in-tube\" Method to Extend Glaucoma Drainage Devices Using Paul Glaucoma Implant.","authors":"Tasmin Berman, Leon Au","doi":"10.5005/jp-journals-10078-1430","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim and background: </strong>To describe a novel and uncomplicated technique of elongating the tubing of a glaucoma drainage device (GDD) sourced from a segment of the tube from a Paul® Glaucoma Implant (PGI).</p><p><strong>Surgical technique: </strong>Conjunctival and Tenon's peritomy are performed with relaxing incisions to expose the original tube. The original tube is then removed from the anterior chamber, and the original entry site is closed. The tip of the original Baerveldt/Ahmed tubing is shortened to near the plate, and the lumen is stretched open using Burke's forceps (nontoothed to avoid damage to the tubing) while the appropriate length of the Paul tube was being pushed inside and is secure without the need for any suturing. The new smaller Paul tube is then inserted back into the anterior chamber using a 26-gauge tract. An 8-0 Ethilon® was then used to secure the tube to the sclera, and TISSEL® was used to secure it (Baxter, United States). Depending on the positioning, either the original Tutoplast® pericardium or new double-layered Tutoplast® can be placed over the tube to prevent erosion. The Tenon's and conjunctiva were then closed to secure the conjunctival and Tenon's back in their original position at the limbus, and the radial conjunctival incisions can be closed using TISSEL® fibrin glue or further sutures if required.</p><p><strong>Conclusion: </strong>This method offers several benefits over previously documented techniques; it avoids significant bulkiness, and the elongated tube conforms to the curvature of the globe owing to the suitable rigidity of the extended section. The additional tubing segment fits securely without the need for sutures. Introducing a smaller diameter tube into the anterior chamber in comparison to other GDDs minimizes the surface area between the tube and corneal endothelium, therefore decreasing the rate of potential endothelium cell loss.</p><p><strong>Clinical significance: </strong>This novel \"tube-in-tube\" technique is efficient, safe, and straightforward to perform. It eliminates the need for alterations in glaucoma medication since the PGI is not thought to offer any flow resistance.</p><p><strong>How to cite this article: </strong>Berman T, Au L. A New \"Tube-in-tube\" Method to Extend Glaucoma Drainage Devices Using Paul Glaucoma Implant. J Curr Glaucoma Pract 2024;18(3):130-133.</p>","PeriodicalId":15419,"journal":{"name":"Journal of Current Glaucoma Practice","volume":"18 3","pages":"130-133"},"PeriodicalIF":0.0000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11576341/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Current Glaucoma Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5005/jp-journals-10078-1430","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/29 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Aim and background: To describe a novel and uncomplicated technique of elongating the tubing of a glaucoma drainage device (GDD) sourced from a segment of the tube from a Paul® Glaucoma Implant (PGI).
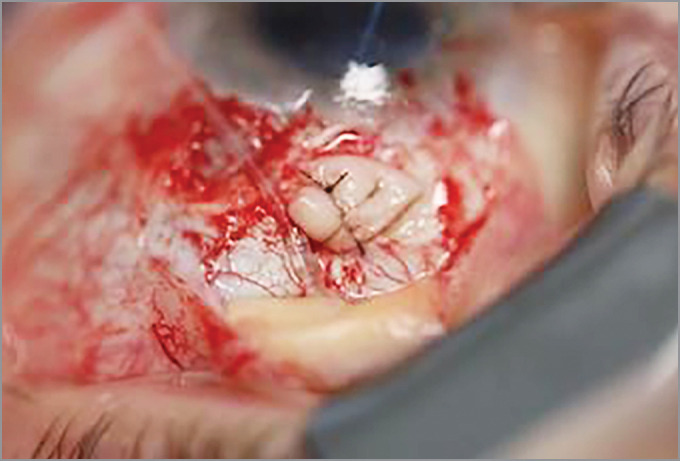
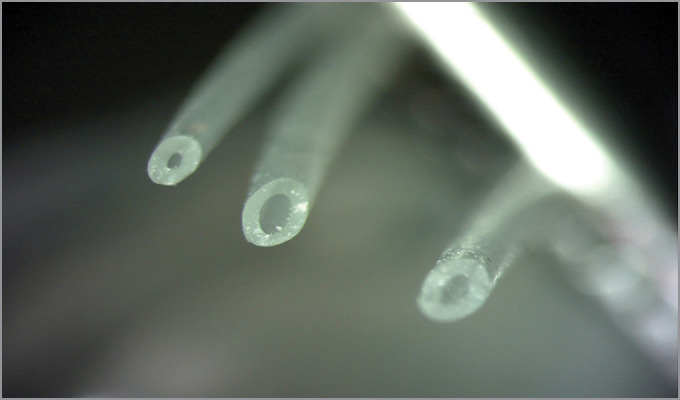
Surgical technique: Conjunctival and Tenon's peritomy are performed with relaxing incisions to expose the original tube. The original tube is then removed from the anterior chamber, and the original entry site is closed. The tip of the original Baerveldt/Ahmed tubing is shortened to near the plate, and the lumen is stretched open using Burke's forceps (nontoothed to avoid damage to the tubing) while the appropriate length of the Paul tube was being pushed inside and is secure without the need for any suturing. The new smaller Paul tube is then inserted back into the anterior chamber using a 26-gauge tract. An 8-0 Ethilon® was then used to secure the tube to the sclera, and TISSEL® was used to secure it (Baxter, United States). Depending on the positioning, either the original Tutoplast® pericardium or new double-layered Tutoplast® can be placed over the tube to prevent erosion. The Tenon's and conjunctiva were then closed to secure the conjunctival and Tenon's back in their original position at the limbus, and the radial conjunctival incisions can be closed using TISSEL® fibrin glue or further sutures if required.
Conclusion: This method offers several benefits over previously documented techniques; it avoids significant bulkiness, and the elongated tube conforms to the curvature of the globe owing to the suitable rigidity of the extended section. The additional tubing segment fits securely without the need for sutures. Introducing a smaller diameter tube into the anterior chamber in comparison to other GDDs minimizes the surface area between the tube and corneal endothelium, therefore decreasing the rate of potential endothelium cell loss.
Clinical significance: This novel "tube-in-tube" technique is efficient, safe, and straightforward to perform. It eliminates the need for alterations in glaucoma medication since the PGI is not thought to offer any flow resistance.
How to cite this article: Berman T, Au L. A New "Tube-in-tube" Method to Extend Glaucoma Drainage Devices Using Paul Glaucoma Implant. J Curr Glaucoma Pract 2024;18(3):130-133.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


