Crystal D Taylor, Ton Wang, Alison S Baskin, Brandy Sinco, Tasha M Hughes, Daniel J Boffa, Judy C Boughey, Lesly A Dossett
{"title":"American College of Surgeons Operative Standards and Breast Cancer Outcomes.","authors":"Crystal D Taylor, Ton Wang, Alison S Baskin, Brandy Sinco, Tasha M Hughes, Daniel J Boffa, Judy C Boughey, Lesly A Dossett","doi":"10.1001/jamanetworkopen.2024.46345","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>The American College of Surgeons (ACS) operative standards were established to detail critical elements of cancer surgery, reduce technical variation, and improve outcomes. Two of the 6 operative standards target adequate axillary surgery for breast cancer. The potential association of the operative standards with short-term oncologic outcomes, such as nodal yield and nodal positivity rates, is currently unknown.</p><p><strong>Objective: </strong>To evaluate the potential association of the ACS operative standards with short-term oncologic outcomes in breast cancer.</p><p><strong>Design, setting, and participants: </strong>A cohort study was performed using data on 1 201 317 women 18 years or older who underwent sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND) for invasive breast cancer from January 1, 2012, to December 31, 2020. Patients were identified using the National Cancer Database (NCDB), a clinical oncology database encompassing approximately 70% of new cancer diagnoses, sourced from hospital registry data from 1317 facilities. Statistical analysis was performed from October 2023 to June 2024.</p><p><strong>Exposure: </strong>Sentinel lymph node biopsy or ALND.</p><p><strong>Main outcomes and measures: </strong>Reliability-adjusted facility-level lymph node yield and nodal positivity rate for each procedure were calculated using generalized linear mixed models, Poisson regression, and logistic regression with facility-level random intercepts.</p><p><strong>Results: </strong>The cohort included 1 201 317 women with a median age of 62 years (IQR, 53-70 years). Facility-level nodal yield ranged from 1 to 6 for SLNB and from 6 to 22 for ALND. Median facility-level nodal yield for SLNB was 2.6 (IQR, 2.3-3.0) and the nodal positivity rate for SLNB was 12.2% (IQR, 11.0%-13.7%), with rates ranging from 6% to 21%. A weak correlation between facility-level lymph node yield and nodal positivity was observed (Spearman correlation coefficient, 0.17). Median nodal upstaging rate (≥4 positive nodes) for ALND was 30.5% (IQR, 26.5%-35.0%), with rates ranging from 11% to 54%; median nodal yield was 12.2 (IQR, 10.9-13.6). A strong correlation between nodal yield and nodal upstaging rates was observed (Spearman correlation coefficient, 0.53).</p><p><strong>Conclusions and relevance: </strong>In this cohort study of women undergoing axillary surgery for invasive breast cancer, facility-level variation in lymph node yield was present for both SLNB and ALND, which could potentially be improved through the ACS operative standards. However, this variation had mixed associations with nodal positivity and upstaging rates, suggesting the association of the ACS operative standards with oncologic outcomes may be mixed.</p>","PeriodicalId":14694,"journal":{"name":"JAMA Network Open","volume":"7 11","pages":"e2446345"},"PeriodicalIF":9.7000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11579798/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Network Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamanetworkopen.2024.46345","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: The American College of Surgeons (ACS) operative standards were established to detail critical elements of cancer surgery, reduce technical variation, and improve outcomes. Two of the 6 operative standards target adequate axillary surgery for breast cancer. The potential association of the operative standards with short-term oncologic outcomes, such as nodal yield and nodal positivity rates, is currently unknown.
Objective: To evaluate the potential association of the ACS operative standards with short-term oncologic outcomes in breast cancer.
Design, setting, and participants: A cohort study was performed using data on 1 201 317 women 18 years or older who underwent sentinel lymph node biopsy (SLNB) or axillary lymph node dissection (ALND) for invasive breast cancer from January 1, 2012, to December 31, 2020. Patients were identified using the National Cancer Database (NCDB), a clinical oncology database encompassing approximately 70% of new cancer diagnoses, sourced from hospital registry data from 1317 facilities. Statistical analysis was performed from October 2023 to June 2024.
Exposure: Sentinel lymph node biopsy or ALND.
Main outcomes and measures: Reliability-adjusted facility-level lymph node yield and nodal positivity rate for each procedure were calculated using generalized linear mixed models, Poisson regression, and logistic regression with facility-level random intercepts.
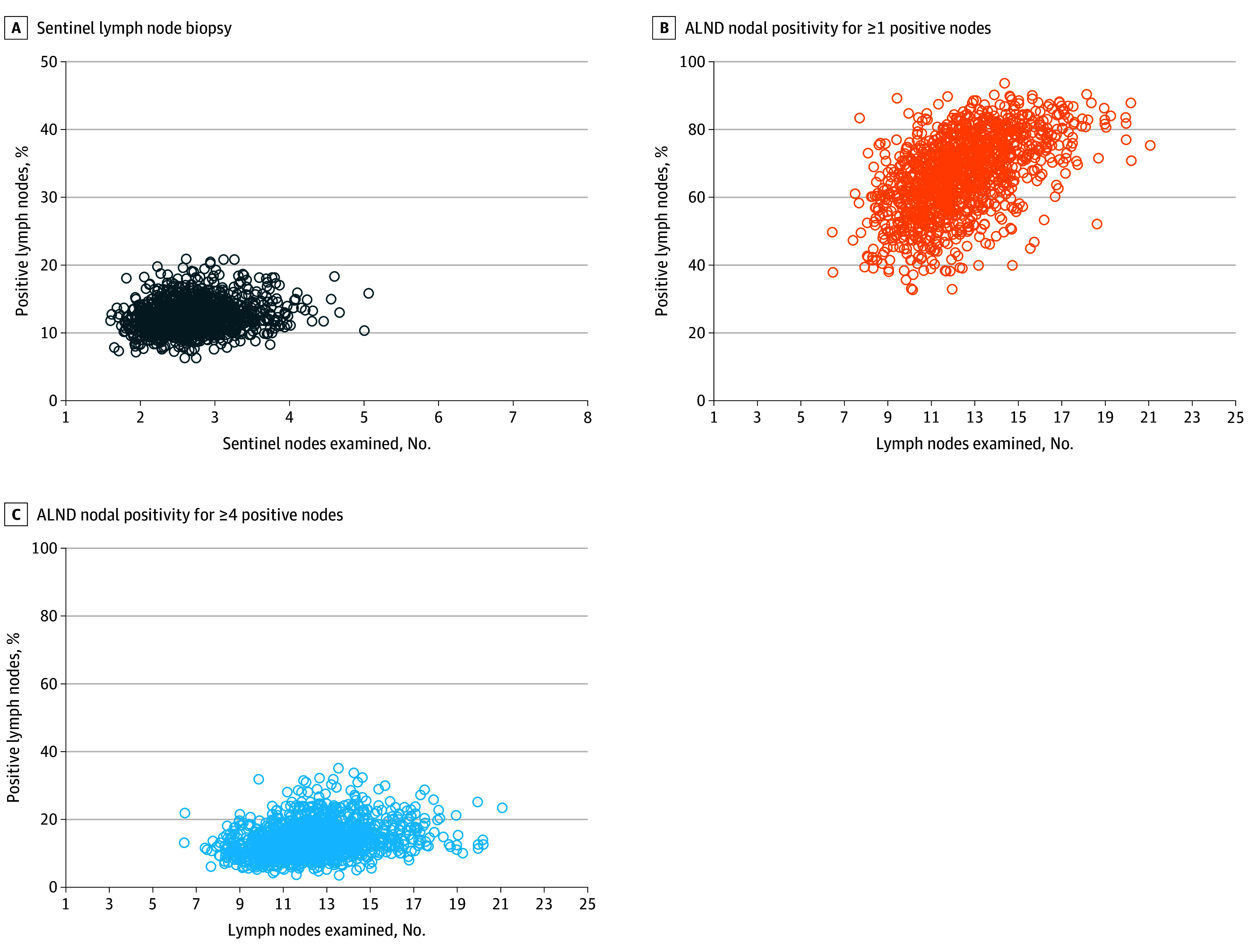
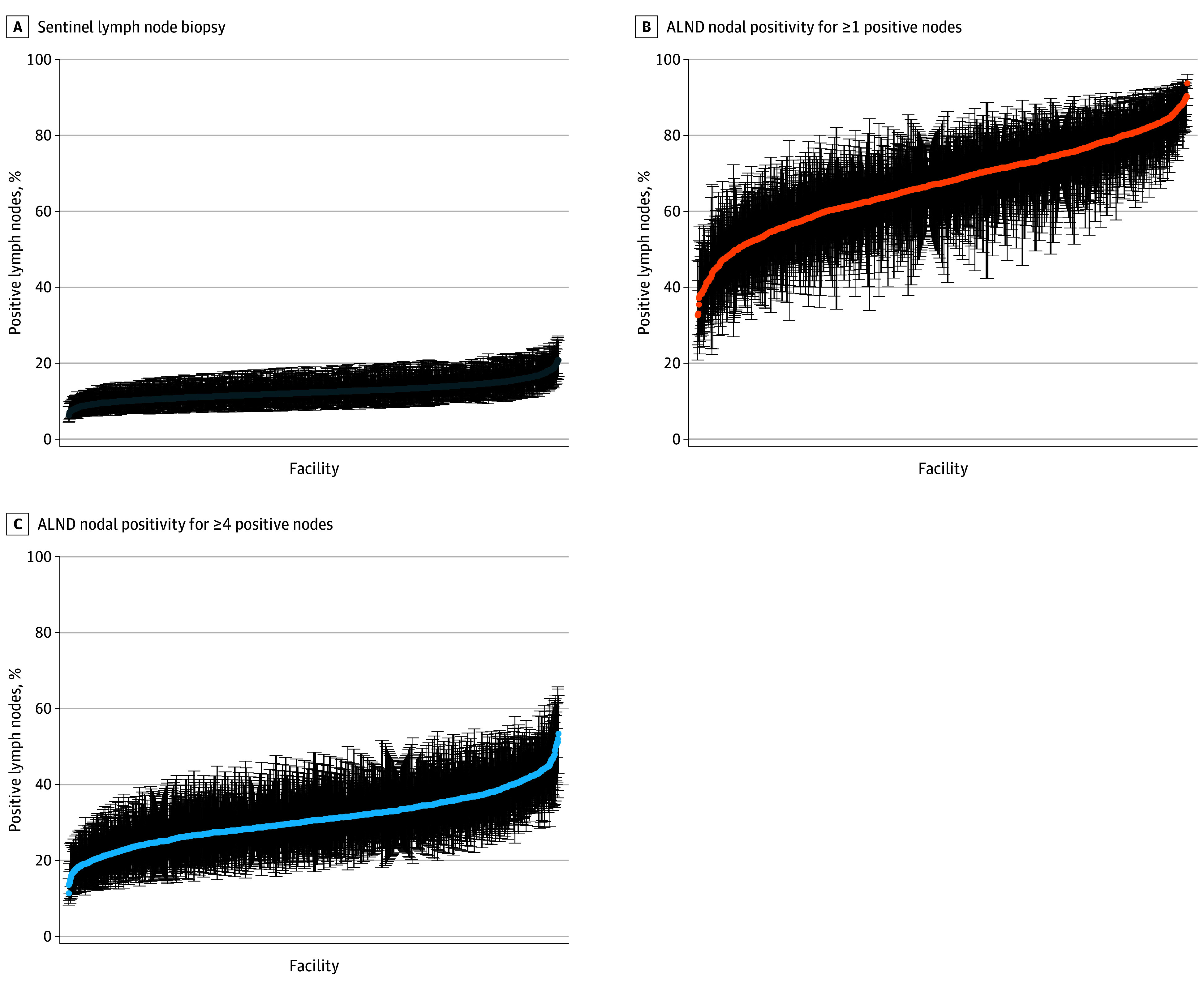
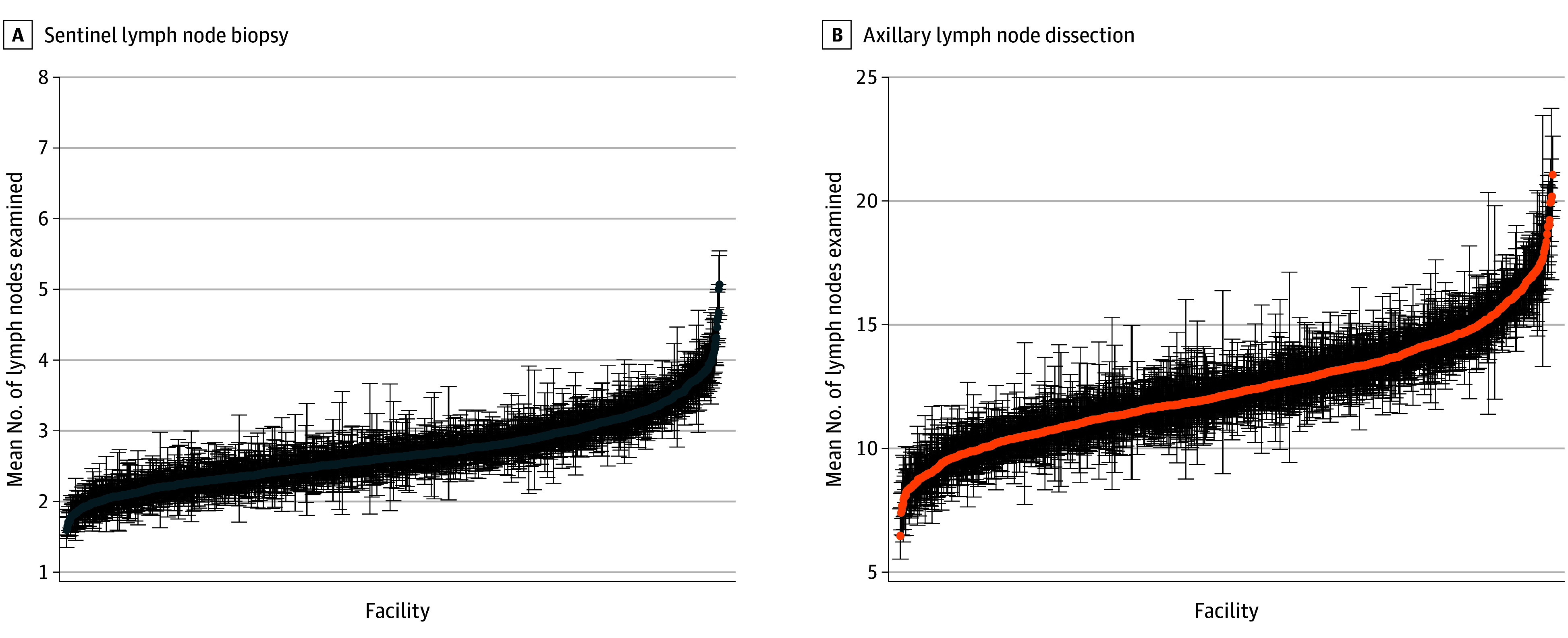
Results: The cohort included 1 201 317 women with a median age of 62 years (IQR, 53-70 years). Facility-level nodal yield ranged from 1 to 6 for SLNB and from 6 to 22 for ALND. Median facility-level nodal yield for SLNB was 2.6 (IQR, 2.3-3.0) and the nodal positivity rate for SLNB was 12.2% (IQR, 11.0%-13.7%), with rates ranging from 6% to 21%. A weak correlation between facility-level lymph node yield and nodal positivity was observed (Spearman correlation coefficient, 0.17). Median nodal upstaging rate (≥4 positive nodes) for ALND was 30.5% (IQR, 26.5%-35.0%), with rates ranging from 11% to 54%; median nodal yield was 12.2 (IQR, 10.9-13.6). A strong correlation between nodal yield and nodal upstaging rates was observed (Spearman correlation coefficient, 0.53).
Conclusions and relevance: In this cohort study of women undergoing axillary surgery for invasive breast cancer, facility-level variation in lymph node yield was present for both SLNB and ALND, which could potentially be improved through the ACS operative standards. However, this variation had mixed associations with nodal positivity and upstaging rates, suggesting the association of the ACS operative standards with oncologic outcomes may be mixed.
期刊介绍:
JAMA Network Open, a member of the esteemed JAMA Network, stands as an international, peer-reviewed, open-access general medical journal.The publication is dedicated to disseminating research across various health disciplines and countries, encompassing clinical care, innovation in health care, health policy, and global health.
JAMA Network Open caters to clinicians, investigators, and policymakers, providing a platform for valuable insights and advancements in the medical field. As part of the JAMA Network, a consortium of peer-reviewed general medical and specialty publications, JAMA Network Open contributes to the collective knowledge and understanding within the medical community.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


