Addition of Sacubitril/Valsartan to Mineralocorticoid Receptor Antagonist Therapy in Primary Aldosteronism: Effects on Plasma Aldosterone Concentration and Plasma Renin Activity.
{"title":"Addition of Sacubitril/Valsartan to Mineralocorticoid Receptor Antagonist Therapy in Primary Aldosteronism: Effects on Plasma Aldosterone Concentration and Plasma Renin Activity.","authors":"Keisuke Okamura, Masatoshi Matsushima, Yosuke Takamiya, Tetsu Okuda, Hideto Sako, Akihiro Udo, Kenichiro Taniguchi, Shogo Morisaki, Ichiro Imamura, Hidenori Urata, Shin-Ichiro Miura","doi":"10.14740/jocmr6058","DOIUrl":null,"url":null,"abstract":"<p><p>In the pharmacologic treatment of primary aldosteronism (PA), titration of mineralocorticoid receptor antagonist (MRA) dosing is necessary to reverse the renin suppression caused by high aldosterone levels. However, we often encounter cases in which the plasma renin activity (PRA) does not achieve the target level, even with the maximum dose of MRA. In this setting, sacubitril/valsartan, a combination of a neprilysin inhibitor and an angiotensin II type 1 receptor blocker that is approved for use as adjunctive therapy with an MRA, has been reported to inhibit aldosterone secretion both <i>in vitro</i> and <i>in vivo</i>. If sacubitril/valsartan proves to be effective in this context, it may offer a promising treatment for PA. However, there are few reports on the use of sacubitril/valsartan in this disease. We used add-on sacubitril/valsartan in three patients with PA, in whom blood pressure was insufficiently reduced and PRA remained suppressed despite administering the maximum dose of MRA. With the addition of sacubitril/valsartan, the decrease in plasma aldosterone concentration (PAC) was more marked than the increase in PRA. Because MRAs do not suppress aldosterone production but instead act by blocking mineralocorticoid receptors, use of these agents actually promotes the renin-angiotensin system and leads to increased PAC resulting from positive feedback. The pathological significance of the phenomenon whereby PAC increases with MRA administration but decreases with the addition of sacubitril/valsartan is unclear. In PA, more effective treatment may be possible by suppressing aldosterone with sacubitril/valsartan and blocking the action of aldosterone with MRAs.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 10","pages":"509-517"},"PeriodicalIF":2.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11557503/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr6058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
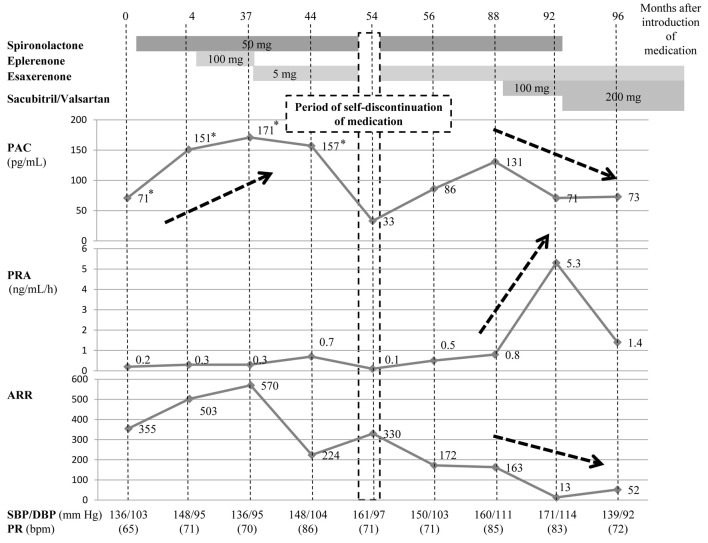
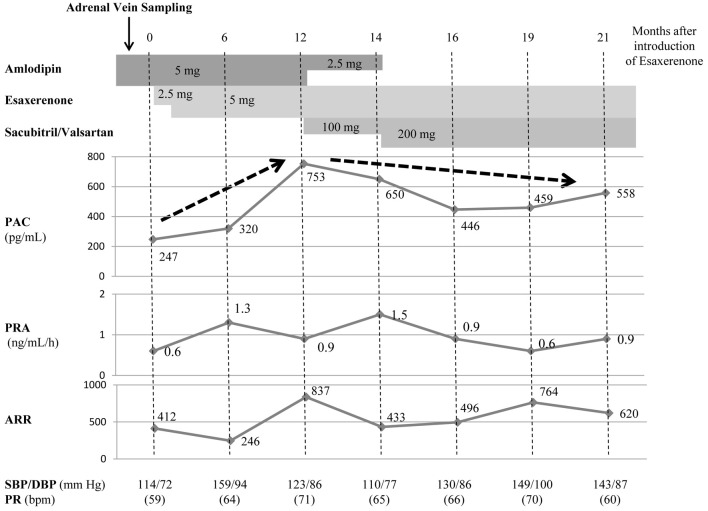
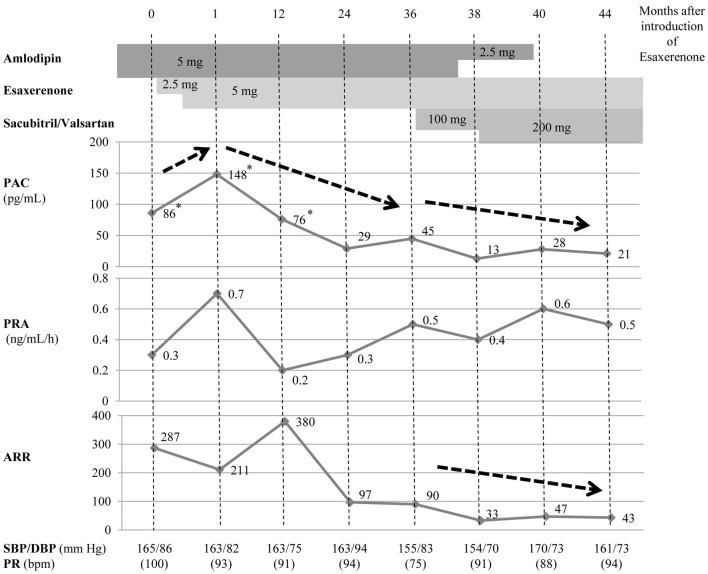
In the pharmacologic treatment of primary aldosteronism (PA), titration of mineralocorticoid receptor antagonist (MRA) dosing is necessary to reverse the renin suppression caused by high aldosterone levels. However, we often encounter cases in which the plasma renin activity (PRA) does not achieve the target level, even with the maximum dose of MRA. In this setting, sacubitril/valsartan, a combination of a neprilysin inhibitor and an angiotensin II type 1 receptor blocker that is approved for use as adjunctive therapy with an MRA, has been reported to inhibit aldosterone secretion both in vitro and in vivo. If sacubitril/valsartan proves to be effective in this context, it may offer a promising treatment for PA. However, there are few reports on the use of sacubitril/valsartan in this disease. We used add-on sacubitril/valsartan in three patients with PA, in whom blood pressure was insufficiently reduced and PRA remained suppressed despite administering the maximum dose of MRA. With the addition of sacubitril/valsartan, the decrease in plasma aldosterone concentration (PAC) was more marked than the increase in PRA. Because MRAs do not suppress aldosterone production but instead act by blocking mineralocorticoid receptors, use of these agents actually promotes the renin-angiotensin system and leads to increased PAC resulting from positive feedback. The pathological significance of the phenomenon whereby PAC increases with MRA administration but decreases with the addition of sacubitril/valsartan is unclear. In PA, more effective treatment may be possible by suppressing aldosterone with sacubitril/valsartan and blocking the action of aldosterone with MRAs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


