Construction and performance of a clinical prediction rule for ureteral stone without the use of race or ethnicity: A new STONE score
Abstract
Objectives
The original STONE score was designed to predict the presence of uncomplicated renal colic and the corresponding absence of alternate serious etiologies. It was retrospectively derived and prospectively validated and resulted in five variables: Sex (male gender), Timing (acute onset of pain), “Origin” (non-Black race), Nausea/vomiting (present), and Erythrocytes (microscopic hematuria). With recent increased awareness of the potential adverse impacts of including race (a socially constructed identity) in clinical prediction rules, we sought to determine if a revised STONE score without race could be constructed with similar diagnostic accuracy.
Methods
We used data from the original STONE score that utilized retrospective data on patients with confirmed kidney stone by computed tomography (CT) to derive a clinical prediction rule as well as prospective data to validate the score. These data were used to construct a revised STONE score after removing race as a variable. We performed univariate and multivariable logistic regression and compared the old and new STONE scores (including multivariable, integral, and three-level risk) using the area under the receiver operating characteristic curve (AUC) and misclassification rates.
Results
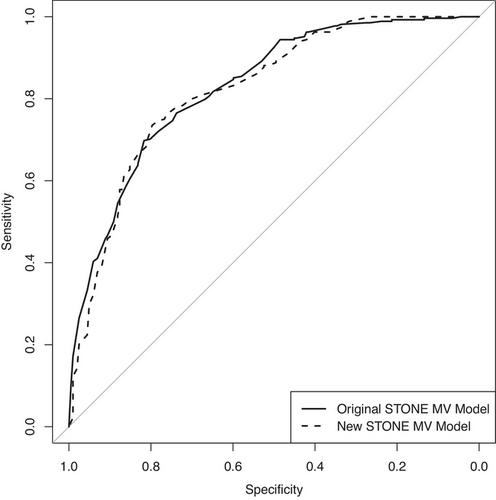
After the elimination of race, multivariable logistic regression revealed that gross hematuria was the next strongest feasible variable for the prediction of ureteral stone. This was incorporated into a revised STONE score by substituting “obvious hematuria” for “origin” (formerly race). The revised STONE score had similar predictive accuracy to the original STONE score: AUC 0.85 versus 0.86 (95% confidence interval [CI]: 0.82–0.87 and 0.79–0.93); misclassification rates were also unchanged, 0.23 versus 0.23 (95% CI: 0.20–0.25 and 0.20–0.25).
Conclusions
We modified the STONE score to remove race and include “obvious hematuria” without losing clinical accuracy. Considering the potential adverse effects of propagating racial bias in clinical algorithms, we recommend using the revised STONE score. Future research could investigate the potential contributions of social drivers of health (SDOH) to the diagnosis of kidney stone.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


