{"title":"Complication of post-lumbar puncture","authors":"Pranjal Rai MBBS, Vasundhara Patil MD","doi":"10.1002/emp2.13308","DOIUrl":null,"url":null,"abstract":"<p>A 17-year-old male with juvenile nasal angiofibroma and intracranial extension underwent tumor excision with dural repair and skull base defect reconstruction using flap, presented with meningismus a year later. Initial computed tomography (CT) scan showed features of meningitis in the form of diffuse sulcal effacement and subtle leptomeningeal enhancement (Figure 1). A lumbar puncture (LP) was performed to obtain cerebral spinal fluid (CSF) for microbiology and biochemical tests. Deterioration of his neurological status approximately 1-week post-procedure prompted an magnetic resonance imaging (MRI) evaluation that revealed multiple susceptibility artifacts on susceptibility-weighted sequences (See Figure 2A and B), which corresponded to pneumocephalus, pneumoventricle, and pneumocistern on CT (See Figure 2C and D). Nasal endoscopy and MRI cisternogram were negative for any fistula. The patient improved symptomatically after 2 weeks with conservative management. Follow-up study showed complete resolution of the findings.</p><p>Initial CT being negative for air (Figure 1), followed by LP-induced pneumocephalus, postulates two possible theories. First is a possible occult, one-way dural fistula at the surgical site leading to slow air entry post-LP into the subarachnoid space due to the over-drainage of CSF, which may have led to intracranial hypotension. This fistula was not detected on the endoscopy or MR cisternogram possibly because the procedures were performed without pressurization of air spaces. The second possibility is accidental injection of air into the subarachnoid space during LP.<span><sup>1</sup></span> Considering the amount of air in this case, the second mechanism appears more likely (See Figure 2</p><p>Subarachnoid pneumocephalus is mostly asymptomatic unless large and resolves spontaneously within 1–2 weeks. Treatment with high concentration of oxygen may also hasten recovery.<span><sup>2</sup></span> While raised intracranial pressure is not an absolute contraindication to lumbar puncture, a controlled drainage with minimum effective amount should be performed in these patients as over-draining CSF may lead to side effects such as post-dural puncture headaches, or air entry into the subarachnoid space through the spinal needle or any indolent surgical site fistula.</p><p>The authors declare no conflicts of interest.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 6","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11543629/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13308","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
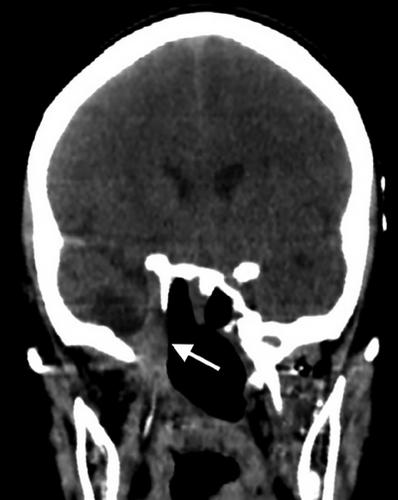
A 17-year-old male with juvenile nasal angiofibroma and intracranial extension underwent tumor excision with dural repair and skull base defect reconstruction using flap, presented with meningismus a year later. Initial computed tomography (CT) scan showed features of meningitis in the form of diffuse sulcal effacement and subtle leptomeningeal enhancement (Figure 1). A lumbar puncture (LP) was performed to obtain cerebral spinal fluid (CSF) for microbiology and biochemical tests. Deterioration of his neurological status approximately 1-week post-procedure prompted an magnetic resonance imaging (MRI) evaluation that revealed multiple susceptibility artifacts on susceptibility-weighted sequences (See Figure 2A and B), which corresponded to pneumocephalus, pneumoventricle, and pneumocistern on CT (See Figure 2C and D). Nasal endoscopy and MRI cisternogram were negative for any fistula. The patient improved symptomatically after 2 weeks with conservative management. Follow-up study showed complete resolution of the findings.
Initial CT being negative for air (Figure 1), followed by LP-induced pneumocephalus, postulates two possible theories. First is a possible occult, one-way dural fistula at the surgical site leading to slow air entry post-LP into the subarachnoid space due to the over-drainage of CSF, which may have led to intracranial hypotension. This fistula was not detected on the endoscopy or MR cisternogram possibly because the procedures were performed without pressurization of air spaces. The second possibility is accidental injection of air into the subarachnoid space during LP.1 Considering the amount of air in this case, the second mechanism appears more likely (See Figure 2
Subarachnoid pneumocephalus is mostly asymptomatic unless large and resolves spontaneously within 1–2 weeks. Treatment with high concentration of oxygen may also hasten recovery.2 While raised intracranial pressure is not an absolute contraindication to lumbar puncture, a controlled drainage with minimum effective amount should be performed in these patients as over-draining CSF may lead to side effects such as post-dural puncture headaches, or air entry into the subarachnoid space through the spinal needle or any indolent surgical site fistula.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


