Katherine I Wolf, Oxana V Crysler, Robert Fontana, Sima Saberi
{"title":"Calcitriol-Mediated Hypercalcemia Due to Liver Metastases in a Patient With Primary Pancreatic Neuroendocrine Tumor.","authors":"Katherine I Wolf, Oxana V Crysler, Robert Fontana, Sima Saberi","doi":"10.1210/jcemcr/luae209","DOIUrl":null,"url":null,"abstract":"<p><p>Hypercalcemia is most commonly associated with primary hyperparathyroidism or malignancy in the setting of elevated parathyroid hormone-related protein or bone metastases. Calcitriol (1,25-dihydroxyvitamin D)-mediated hypercalcemia is rare and typically associated with granulomatous conditions; however, other solid-organ etiologies have been reported. Here, we detail the case of a 62-year-old man with metastatic pancreatic neuroendocrine tumor (pNET) with hypercalcemia refractory to traditional bisphosphonate therapy in the setting of vastly elevated 1,25-dihydroxyvitamin D. Only after initiation of chemotherapy with capecitabine and temozolomide did his serum calcium consistently improve and 1,25-dihydroxyvitamin D begin to decrease. There are fewer than 5 reported cases of a pNET resulting in calcitriol-mediated hypercalcemia. Prompt initiation of treatment for the underlying condition can result in a significant improvement in serum calcium or 1,25-dihydroxyvitamin D. Multiple reports have also demonstrated success with high-dose steroid administration in patients with other solid-organ etiologies of calcitriol-mediated hypercalcemia, but this has not yet been reviewed in the pNET population.</p>","PeriodicalId":73540,"journal":{"name":"JCEM case reports","volume":"2 12","pages":"luae209"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11561906/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JCEM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jcemcr/luae209","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
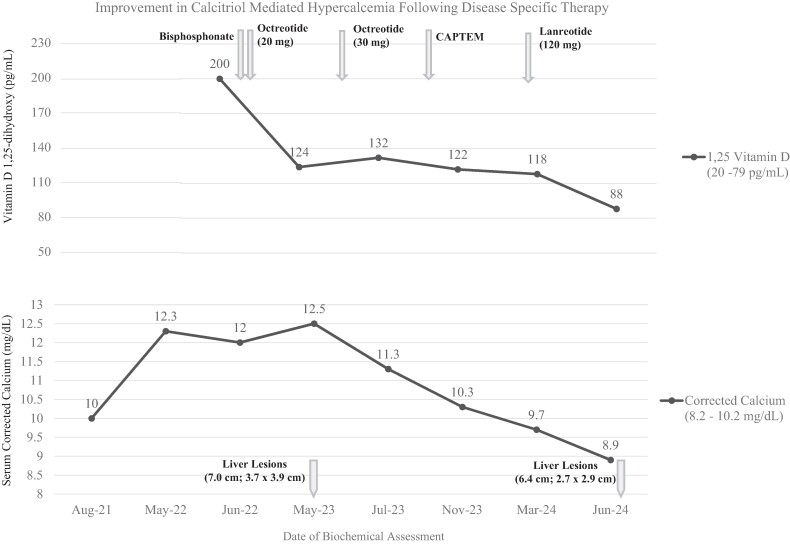
Hypercalcemia is most commonly associated with primary hyperparathyroidism or malignancy in the setting of elevated parathyroid hormone-related protein or bone metastases. Calcitriol (1,25-dihydroxyvitamin D)-mediated hypercalcemia is rare and typically associated with granulomatous conditions; however, other solid-organ etiologies have been reported. Here, we detail the case of a 62-year-old man with metastatic pancreatic neuroendocrine tumor (pNET) with hypercalcemia refractory to traditional bisphosphonate therapy in the setting of vastly elevated 1,25-dihydroxyvitamin D. Only after initiation of chemotherapy with capecitabine and temozolomide did his serum calcium consistently improve and 1,25-dihydroxyvitamin D begin to decrease. There are fewer than 5 reported cases of a pNET resulting in calcitriol-mediated hypercalcemia. Prompt initiation of treatment for the underlying condition can result in a significant improvement in serum calcium or 1,25-dihydroxyvitamin D. Multiple reports have also demonstrated success with high-dose steroid administration in patients with other solid-organ etiologies of calcitriol-mediated hypercalcemia, but this has not yet been reviewed in the pNET population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


