The accuracy of ultrasensitive PSA in predicting disease progression after radical prostatectomy
Abstract
Objectives
To assess the role of ultrasensitive PSA values (usPSA) after radical prostatectomy in predicting the subsequent biochemical recurrence (BCR).
Material and methods
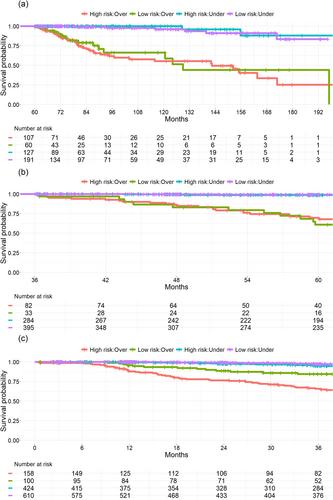
The study included 1836 patients who underwent open or robot-assisted RP at Turku University Hospital between 2003 and 2018. Exclusion criteria involved patients with adjuvant treatments and those who did not reach a PSA nadir <0.1 ng/ml, resulting in a final cohort of 1313 patients. The prognostic impact of the optimal usPSA nadir cut-off value 6 months after RP was investigated to predict subsequent BCR for the whole cohort (N = 1313). The optimal usPSA cut-off value was determined for patients at 3–5 years post-surgery (N = 806) and beyond 5 years (N = 493) of follow-up. We used the area under the curve (AUC) calculation and the Kaplan–Meier method.
Results
In a cohort with a median age of 64, primarily featuring Gleason score 7 prostate cancer. uPSA nadir of 0.01 ng/ml (AUC = 0.80) at the first monitoring post-surgery emerged as the optimal cut-off for identifying subjects at low (80%) or high (20%) risk of BCR within the first 3 years. Beyond this period, uPSA values during the first 3 [(AUC = 0.89; 3–5 years post-surgery) and (AUC = 0.81; beyond 5 years)] and 5 post-surgery years (AUC = 0.85) outperformed uPSA nadir in predicting subsequent BCR. Notably, EAU-defined high-risk patients with low uPSA nadir maintained substantial BCR-free survival.
Conclusion
In conclusion, a low usPSA predicts minimal BCR risk over the next 2–3 years post-measurement. Patients with low usPSA can benefit from reduced post-surgery PSA monitoring at 2- to 3-year intervals without compromising outcomes. This strategic approach optimizes resource allocation in busy urological outpatient clinics, especially valuable in publicly reimbursed healthcare systems like Finland.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


