Population-level health impact of hypothetical waning 1-dose human papillomavirus vaccination and 2-dose mitigation strategies in a high cervical cancer burden setting.
Emily A Burger, Jean-François Laprise, Allison Portnoy, Jennifer C Spencer, Stephen Sy, Mary Caroline Regan, Élodie Bénard, Mélanie Drolet, Marc Brisson, Jane J Kim
{"title":"Population-level health impact of hypothetical waning 1-dose human papillomavirus vaccination and 2-dose mitigation strategies in a high cervical cancer burden setting.","authors":"Emily A Burger, Jean-François Laprise, Allison Portnoy, Jennifer C Spencer, Stephen Sy, Mary Caroline Regan, Élodie Bénard, Mélanie Drolet, Marc Brisson, Jane J Kim","doi":"10.1093/jncimonographs/lgae039","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We simulated the impact of hypothetical waning scenarios of a 1-dose human papillomavirus (HPV) vaccination paired with switching to 2-dose mitigation strategies guided by empirical vaccine trial reporting timelines.</p><p><strong>Methods: </strong>Using 2 independent mathematical models fitted to a high-burden setting, we projected the cumulative cervical cancer cases averted over 85 years for alternative HPV vaccination scenarios under 2 program adoption timelines: 1) de novo introduction of a 1-dose HPV vaccination and 2) a switch from an existing 2-dose HPV vaccination program to a 1-dose vaccination. We assumed 80% vaccination coverage with the bivalent vaccine and an average duration of a 1-dose HPV vaccine protection of either 30 or 25 years with 100% efficacy. We varied the eligible age group(s) at program introduction and the 2-dose mitigation (single-age cohort or multi-age cohort). If needed for mitigation, reintroduction of 2-dose vaccination was assumed to occur in 2036 (ie, 30 years after initiation of the Costa Rica Vaccine Trial).</p><p><strong>Results: </strong>Under both vaccine adoption timelines, the models projected that countries could achieve the same level of health benefits by switching to 2 doses in 2036 using a multi-age cohort approach as with initiating a 2-dose or 1-dose vaccination program with no waning. With only a single-age cohort 2-dose mitigation approach, 98%-99% of cases would be prevented compared with the health benefits of 2 doses or a noninferior, durable 1 dose.</p><p><strong>Conclusions: </strong>Countries hesitant to adopt a 1-dose HPV vaccination program may have opportunities to leverage the benefits and efficiency of a 1-dose schedule while awaiting longer-term reporting from 1-dose durability studies, including Costa Rica Vaccine Trial.</p>","PeriodicalId":73988,"journal":{"name":"Journal of the National Cancer Institute. Monographs","volume":"2024 67","pages":"379-386"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11555273/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the National Cancer Institute. Monographs","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jncimonographs/lgae039","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We simulated the impact of hypothetical waning scenarios of a 1-dose human papillomavirus (HPV) vaccination paired with switching to 2-dose mitigation strategies guided by empirical vaccine trial reporting timelines.
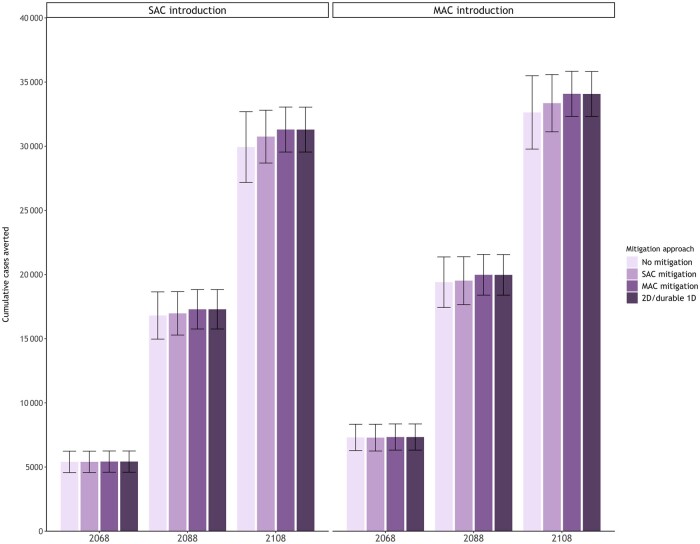
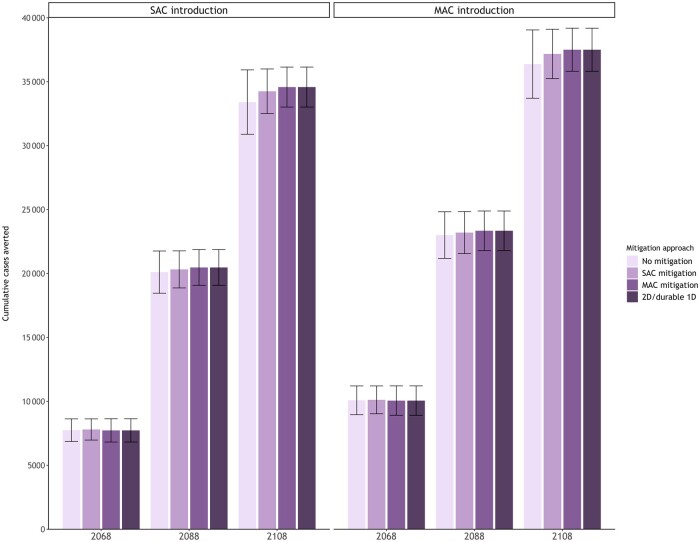
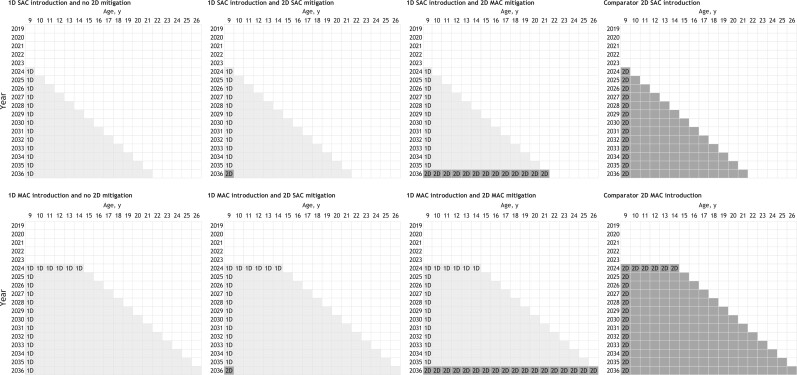
Methods: Using 2 independent mathematical models fitted to a high-burden setting, we projected the cumulative cervical cancer cases averted over 85 years for alternative HPV vaccination scenarios under 2 program adoption timelines: 1) de novo introduction of a 1-dose HPV vaccination and 2) a switch from an existing 2-dose HPV vaccination program to a 1-dose vaccination. We assumed 80% vaccination coverage with the bivalent vaccine and an average duration of a 1-dose HPV vaccine protection of either 30 or 25 years with 100% efficacy. We varied the eligible age group(s) at program introduction and the 2-dose mitigation (single-age cohort or multi-age cohort). If needed for mitigation, reintroduction of 2-dose vaccination was assumed to occur in 2036 (ie, 30 years after initiation of the Costa Rica Vaccine Trial).
Results: Under both vaccine adoption timelines, the models projected that countries could achieve the same level of health benefits by switching to 2 doses in 2036 using a multi-age cohort approach as with initiating a 2-dose or 1-dose vaccination program with no waning. With only a single-age cohort 2-dose mitigation approach, 98%-99% of cases would be prevented compared with the health benefits of 2 doses or a noninferior, durable 1 dose.
Conclusions: Countries hesitant to adopt a 1-dose HPV vaccination program may have opportunities to leverage the benefits and efficiency of a 1-dose schedule while awaiting longer-term reporting from 1-dose durability studies, including Costa Rica Vaccine Trial.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


