{"title":"Real-World Experience of the Association of HLADQA1*05 Allele With Loss of Response to Anti-TNF Inhibitors.","authors":"Aastha Chokshi, Christina A Raker, Sean Fine","doi":"10.1093/crocol/otae058","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antitumor necrosis factor (anti-TNF) biologics have revolutionized the treatment of inflammatory bowel disease (IBD). Previously, studies have shown an association between the HLADQA1*05 allele and the development of antibodies and were predictive of loss of response. We sought to investigate the rate of the HLADQA1*05 allele in patients with IBD at a New England center and its association with antibody development and discontinuation of anti-TNF therapy.</p><p><strong>Methods: </strong>A single center retrospective cohort study with patients on anti-TNF inhibitor therapy being followed at our IBD clinic who had testing performed for the HLADQA1*05 allele were identified and separated into 2 different groups: HLADQA1*05 positive (HLA carriers) or HLADQA1*05 negative (HLA noncarriers). Persistence of remaining on anti-TNF therapy, measurement of drug/antibody levels, and need for dose escalation were collected and stratified amongst the 2 groups.</p><p><strong>Results: </strong>The prevalence of the HLADQA1*05 allele among all IBD patients followed was 53%. We identified 67 IBD patients being treated with anti-TNF medications, 46 (69%) patients with Crohn's disease and 21 (31%) with ulcerative colitis. Most of the HLA carriers (85%) and HLA noncarriers (92%) remained on anti-TNF therapy at the end of the study period. Thirty-six (84%) patients had therapeutic drug monitoring performed during maintenance therapy. Three patients in the HLA carrier group had meaningful antidrug antibody levels necessitating cessation of therapy compared to one patient in the HLA noncarrier group (<i>P</i> = .61). Only 3 (13%) of HLA carriers and 4 (21%) of HLA noncarriers were on combination therapy with an immunomodulator. 65% of HLA carriers required dose escalation compared to 50% of HLA noncarriers (<i>P</i> = .70).</p><p><strong>Conclusions: </strong>The prevalence of the HLADQA1*05 allele was 53% in our New England IBD patient population, similar to what has previously been reported in European studies. The majority of patients remained on anti-TNF therapy at the end of the study period despite carrier status. While there was a trend toward increased need for dose escalation among HLA carriers, this was not statistically significant. Future studies are needed to determine if the presence of the HLADQA1*05 allele leads to antibody development against anti-TNF inhibitors and treatment failure in patients with IBD.</p>","PeriodicalId":10847,"journal":{"name":"Crohn's & Colitis 360","volume":"6 4","pages":"otae058"},"PeriodicalIF":1.8000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11549495/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Crohn's & Colitis 360","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/crocol/otae058","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Antitumor necrosis factor (anti-TNF) biologics have revolutionized the treatment of inflammatory bowel disease (IBD). Previously, studies have shown an association between the HLADQA1*05 allele and the development of antibodies and were predictive of loss of response. We sought to investigate the rate of the HLADQA1*05 allele in patients with IBD at a New England center and its association with antibody development and discontinuation of anti-TNF therapy.
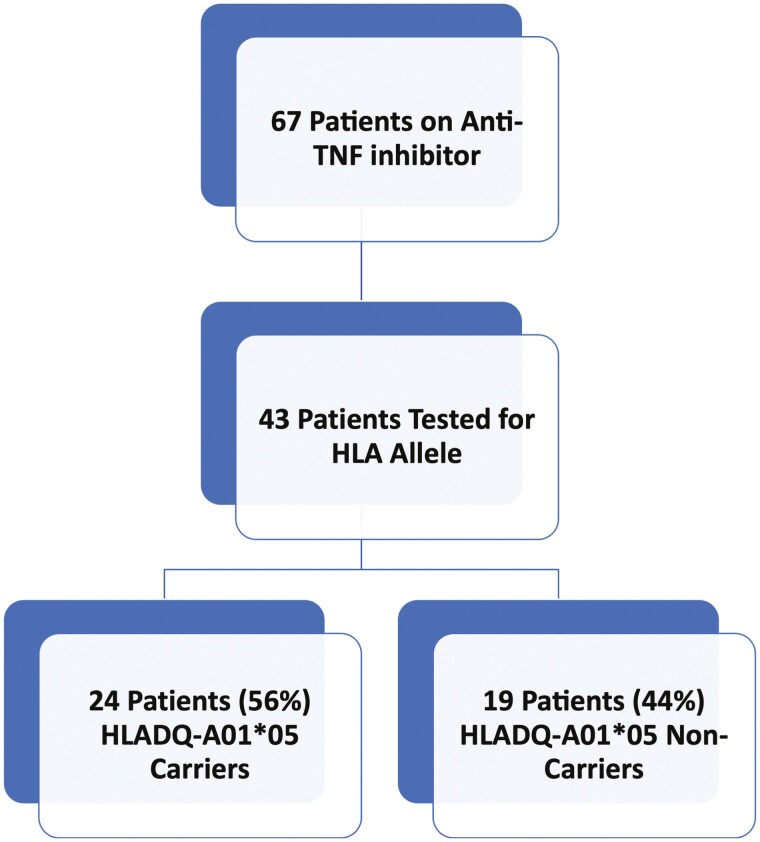
Methods: A single center retrospective cohort study with patients on anti-TNF inhibitor therapy being followed at our IBD clinic who had testing performed for the HLADQA1*05 allele were identified and separated into 2 different groups: HLADQA1*05 positive (HLA carriers) or HLADQA1*05 negative (HLA noncarriers). Persistence of remaining on anti-TNF therapy, measurement of drug/antibody levels, and need for dose escalation were collected and stratified amongst the 2 groups.
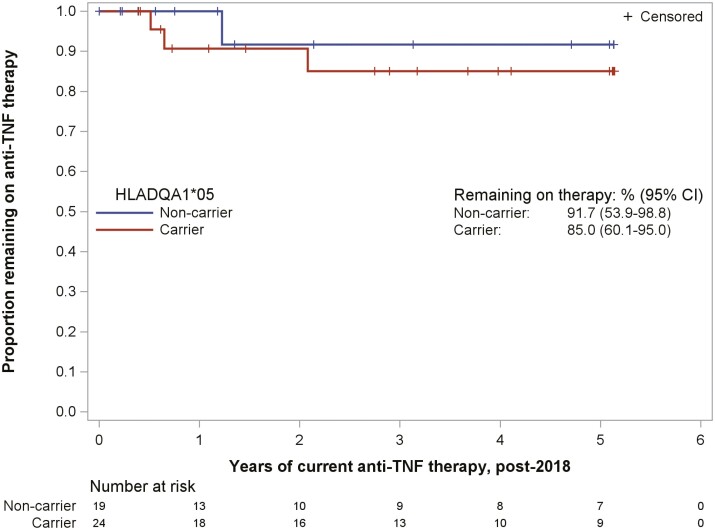
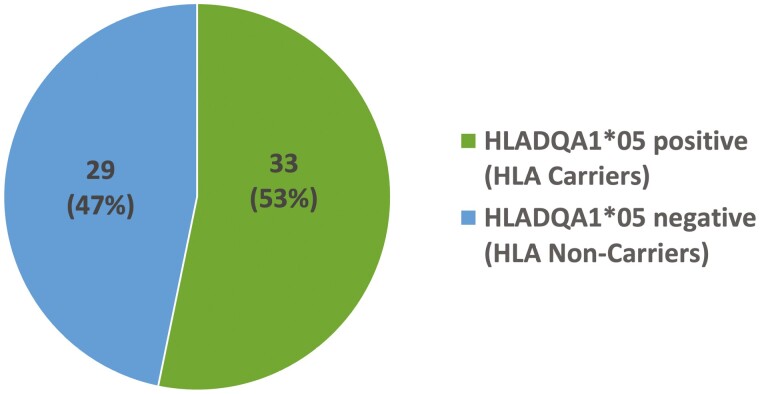
Results: The prevalence of the HLADQA1*05 allele among all IBD patients followed was 53%. We identified 67 IBD patients being treated with anti-TNF medications, 46 (69%) patients with Crohn's disease and 21 (31%) with ulcerative colitis. Most of the HLA carriers (85%) and HLA noncarriers (92%) remained on anti-TNF therapy at the end of the study period. Thirty-six (84%) patients had therapeutic drug monitoring performed during maintenance therapy. Three patients in the HLA carrier group had meaningful antidrug antibody levels necessitating cessation of therapy compared to one patient in the HLA noncarrier group (P = .61). Only 3 (13%) of HLA carriers and 4 (21%) of HLA noncarriers were on combination therapy with an immunomodulator. 65% of HLA carriers required dose escalation compared to 50% of HLA noncarriers (P = .70).
Conclusions: The prevalence of the HLADQA1*05 allele was 53% in our New England IBD patient population, similar to what has previously been reported in European studies. The majority of patients remained on anti-TNF therapy at the end of the study period despite carrier status. While there was a trend toward increased need for dose escalation among HLA carriers, this was not statistically significant. Future studies are needed to determine if the presence of the HLADQA1*05 allele leads to antibody development against anti-TNF inhibitors and treatment failure in patients with IBD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


