{"title":"Association of Smoking with Chronic Kidney Disease Stages 3 to 5: A Mendelian Randomization Study.","authors":"Zhilong Zhang, Feifei Zhang, Xiaomeng Zhang, Lanlan Lu, Luxia Zhang","doi":"10.34133/hds.0199","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Previous studies suggested that smoking behavior (e.g., smoking status) was associated with an elevated risk of chronic kidney disease (CKD), yet whether this association is causal remains uncertain. <b>Methods:</b> We used data for half million participants aged 40 to 69 years from the UK Biobank cohort. In the traditional observational study, we used Cox proportional hazards models to calculate the associations between 2 smoking indices-smoking status and lifetime smoking index and incident CKD stages 3 to 5. Mendelian randomization (MR) approaches were used to estimate a potential causal effect. In one-sample MR, genetic variants associated with lifetime smoking index were used as instrument variables to examine the causal associations with CKD stages 3 to 5, among 344,255 UK Biobank participants with white British ancestry. We further validated our findings by a two-sample MR analysis using information from the Chronic Kidney Disease Genetics Consortium genome-wide association study. <b>Results:</b> In the traditional observational study, both smoking status [hazard ratio (HR): 1.26, 95% confidence interval (CI): 1.22 to 1.30] and lifetime smoking index (HR: 1.22, 95% CI: 1.20 to 1.24) were positively associated with a higher risk of incident CKD. However, both our one-sample and two-sample MR analyses showed no causal association between lifetime smoking index and CKD (all <i>P</i> > 0.05). The genetic instruments were validated by several statistical tests, and all sensitivity analyses showed similar results with the main model. <b>Conclusion:</b> Evidence from our analyses does not suggest a causal effect of smoking behavior on CKD risk. The positive association presented in the traditional observational study is possibly a result of confounding.</p>","PeriodicalId":73207,"journal":{"name":"Health data science","volume":"4 ","pages":"0199"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11532587/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Health data science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34133/hds.0199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
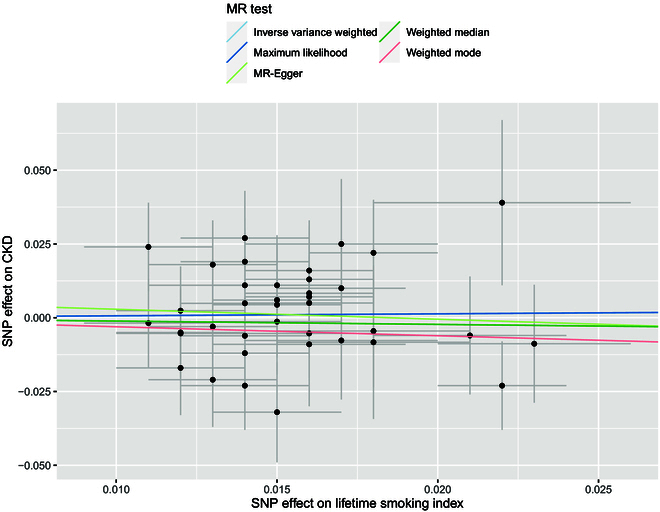
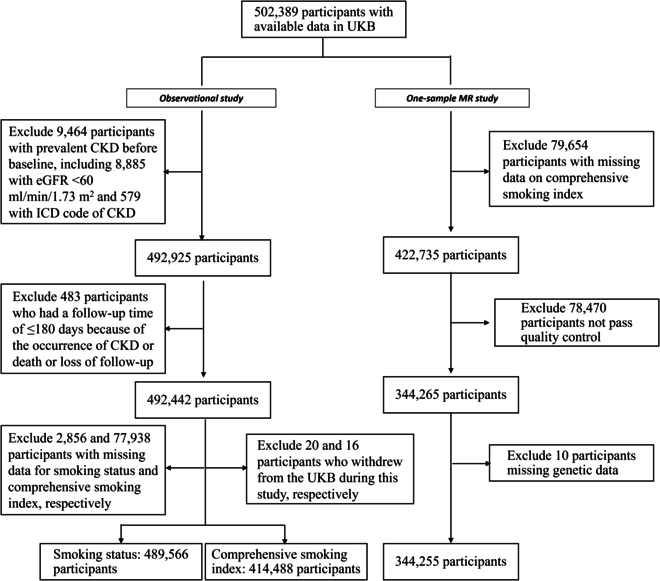
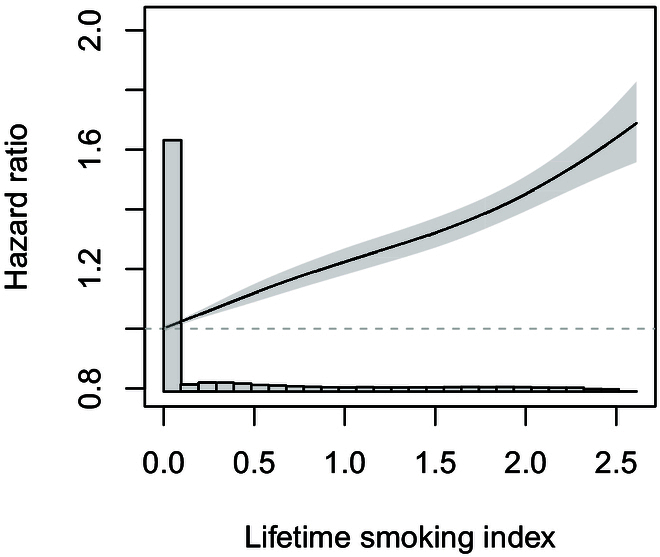
Background: Previous studies suggested that smoking behavior (e.g., smoking status) was associated with an elevated risk of chronic kidney disease (CKD), yet whether this association is causal remains uncertain. Methods: We used data for half million participants aged 40 to 69 years from the UK Biobank cohort. In the traditional observational study, we used Cox proportional hazards models to calculate the associations between 2 smoking indices-smoking status and lifetime smoking index and incident CKD stages 3 to 5. Mendelian randomization (MR) approaches were used to estimate a potential causal effect. In one-sample MR, genetic variants associated with lifetime smoking index were used as instrument variables to examine the causal associations with CKD stages 3 to 5, among 344,255 UK Biobank participants with white British ancestry. We further validated our findings by a two-sample MR analysis using information from the Chronic Kidney Disease Genetics Consortium genome-wide association study. Results: In the traditional observational study, both smoking status [hazard ratio (HR): 1.26, 95% confidence interval (CI): 1.22 to 1.30] and lifetime smoking index (HR: 1.22, 95% CI: 1.20 to 1.24) were positively associated with a higher risk of incident CKD. However, both our one-sample and two-sample MR analyses showed no causal association between lifetime smoking index and CKD (all P > 0.05). The genetic instruments were validated by several statistical tests, and all sensitivity analyses showed similar results with the main model. Conclusion: Evidence from our analyses does not suggest a causal effect of smoking behavior on CKD risk. The positive association presented in the traditional observational study is possibly a result of confounding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


