Ilya A Soynov, Ksenya A Rzayeva, Yuriy N Gorbatykh, Yuriy Y Kulyabin, Artem V Gorbatykh, Ilya A Velyukhanov, Nataliya R Nichay, Serezha N Manukian, Saihuna A Magbulova, Aleksey N Arkhipov, Aleksander V Bogachev-Prokophiev
{"title":"Comparison of Sternotomy Access Versus Thoracotomy Access in the Surgical Treatment of Aortic Coarctation: A Propensity Score-matched Study.","authors":"Ilya A Soynov, Ksenya A Rzayeva, Yuriy N Gorbatykh, Yuriy Y Kulyabin, Artem V Gorbatykh, Ilya A Velyukhanov, Nataliya R Nichay, Serezha N Manukian, Saihuna A Magbulova, Aleksey N Arkhipov, Aleksander V Bogachev-Prokophiev","doi":"10.37616/2212-5043.1396","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The search for the \"Holy Grail\" of surgical repair for aortic coarctation involves finding an access and correction method that successfully and consistently avoids aortic recoarctation and arterial hypertension. The controversy persists as there is still no consensus on the best surgical approach and technique to achieve these objectives.</p><p><strong>Objective: </strong>The objective of this study is to compare sternotomy and left thoracotomy as surgical techniques for treating patients with aortic coarctation and hypoplasia of the distal aortic arch.</p><p><strong>Methods: </strong>From January 2008 to December 2020, 103 surgical procedures were performed using an extended oblique anastomosis. The patients were divided into 2 groups: oblique, extended anastomosis from thoracotomy access (n-68; 66%) and oblique extended anastomosis from sternotomy access (n-35; 34%). After performing a propensity score analysis (1:1) for the entire sample, 25 patients from sternotomy access were matched with 25 patients from thoracotomy access.</p><p><strong>Results: </strong>The mortality rate in the thoracotomy group was 4%, with 1 patient, while it was 8% with 2 patients in the sternotomy group, p > 0.99. There were no significant differences in early postoperative complications between the two groups. Recurrence of aortic coarctation was observed more frequently in the thoracotomy group (20.8% vs 0%). Low weight was identified as the only risk factor for aortic re-coarctation.</p><p><strong>Conclusion: </strong>The mortality rates and early postoperative complications associated with the surgical repair of aortic coarctation were similar between the sternotomy and thoracotomy approaches. Nevertheless, sternotomy approach may be beneficial in reducing aortic recoarctation.</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"36 3","pages":"305-315"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534338/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1396","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The search for the "Holy Grail" of surgical repair for aortic coarctation involves finding an access and correction method that successfully and consistently avoids aortic recoarctation and arterial hypertension. The controversy persists as there is still no consensus on the best surgical approach and technique to achieve these objectives.
Objective: The objective of this study is to compare sternotomy and left thoracotomy as surgical techniques for treating patients with aortic coarctation and hypoplasia of the distal aortic arch.
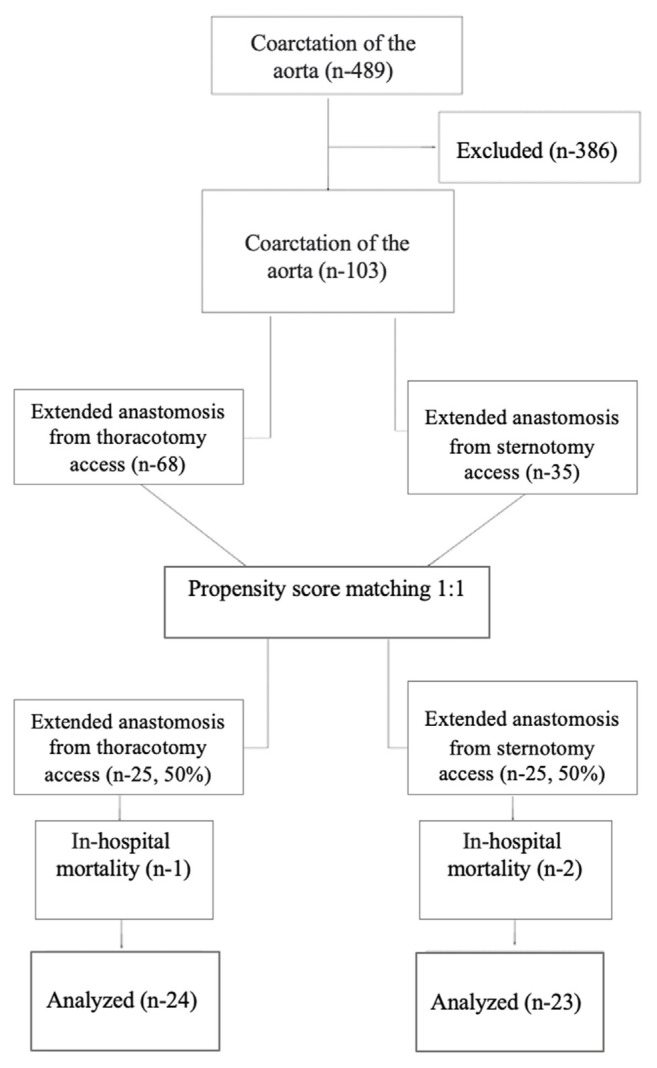
Methods: From January 2008 to December 2020, 103 surgical procedures were performed using an extended oblique anastomosis. The patients were divided into 2 groups: oblique, extended anastomosis from thoracotomy access (n-68; 66%) and oblique extended anastomosis from sternotomy access (n-35; 34%). After performing a propensity score analysis (1:1) for the entire sample, 25 patients from sternotomy access were matched with 25 patients from thoracotomy access.
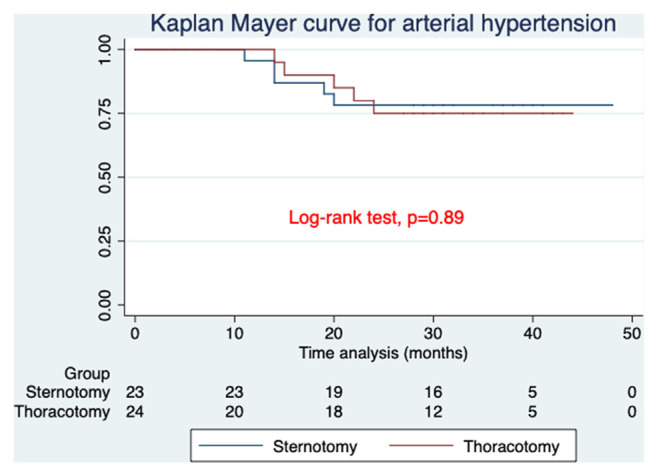
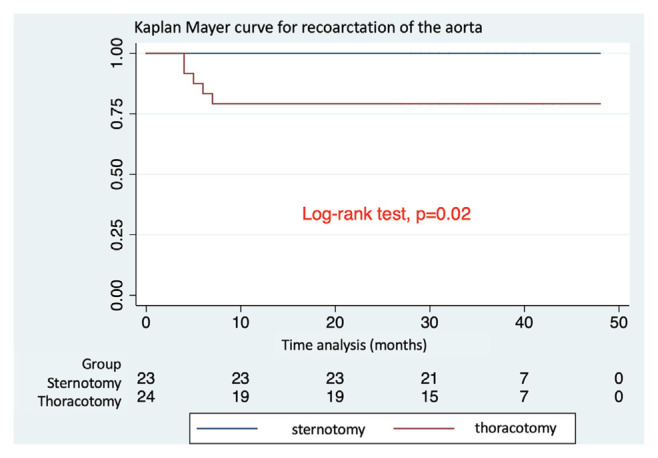
Results: The mortality rate in the thoracotomy group was 4%, with 1 patient, while it was 8% with 2 patients in the sternotomy group, p > 0.99. There were no significant differences in early postoperative complications between the two groups. Recurrence of aortic coarctation was observed more frequently in the thoracotomy group (20.8% vs 0%). Low weight was identified as the only risk factor for aortic re-coarctation.
Conclusion: The mortality rates and early postoperative complications associated with the surgical repair of aortic coarctation were similar between the sternotomy and thoracotomy approaches. Nevertheless, sternotomy approach may be beneficial in reducing aortic recoarctation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


