Matteo Dalmazzo, Melissa Padrini, Sofia Camerlo, Giorgio Rosati, Tiziano Tommaso Busana, Paolo Nicoli, Fabio Perotto, Luca Davicco, Pietro Caironi, Marco De Gobbi, Alessandro Morotti
{"title":"Scedosporium Brain Abscess: A Rare and Fatal Drawback of Bruton Tyrosine Kinase Inhibitor Therapy.","authors":"Matteo Dalmazzo, Melissa Padrini, Sofia Camerlo, Giorgio Rosati, Tiziano Tommaso Busana, Paolo Nicoli, Fabio Perotto, Luca Davicco, Pietro Caironi, Marco De Gobbi, Alessandro Morotti","doi":"10.14740/jh1263","DOIUrl":null,"url":null,"abstract":"<p><p>The patient described in this case report was admitted to the San Luigi Hospital in Turin for confusion, drowsiness, and buccal and eye deviation. An acute neurological disease was suspected. He was affected by chronic lymphocytic leukemia (CLL) on active treatment with the novel Bruton tyrosine kinase inhibitor (BTKi) acalabrutinib. Other comorbidities included type II diabetes mellitus, arterial hypertension, and nonalcoholic steatohepatitis. Imaging exams showed multiple brain lesions, which appeared to be of infectious-inflammatory origin. Consequently, therapy with acalabrutinib was withheld. The patient was later transferred to the intensive care unit, because of worsening neurological conditions. The definite diagnosis of fungal abscess was obtained through a stereotactic biopsy of the widest brain lesion. Microbiological tests confirmed Scedosporium spp. as the etiological agent. Once a detailed antibiogram had been obtained, voriconazole therapy was started. However, the patient's clinical conditions decayed rapidly and he later died of neurological complications. BTKis represent a milestone in the treatment of CLL; however, little is known about how these molecules act on the immune system. Fungal brain abscesses are rare conditions more commonly seen in heavily immunocompromised patients, such as those affected by acquired immune deficiency syndrome, after bone marrow transplant or treatment for acute leukemia. Whether or not therapy with BTKis can favor opportunistic fungal infections is still a matter of debate. Various reports of Aspergillosis infections developing after therapy with ibrutinib exist. Evidence does suggest that an iatrogenic impairment in the innate immune system could favor these infections. In addition, the patient's comorbidities, such as diabetes mellitus and advancing hematological disease, might create the ideal breeding ground for these microorganisms.</p>","PeriodicalId":15964,"journal":{"name":"Journal of hematology","volume":"13 5","pages":"224-228"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11526582/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jh1263","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/21 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
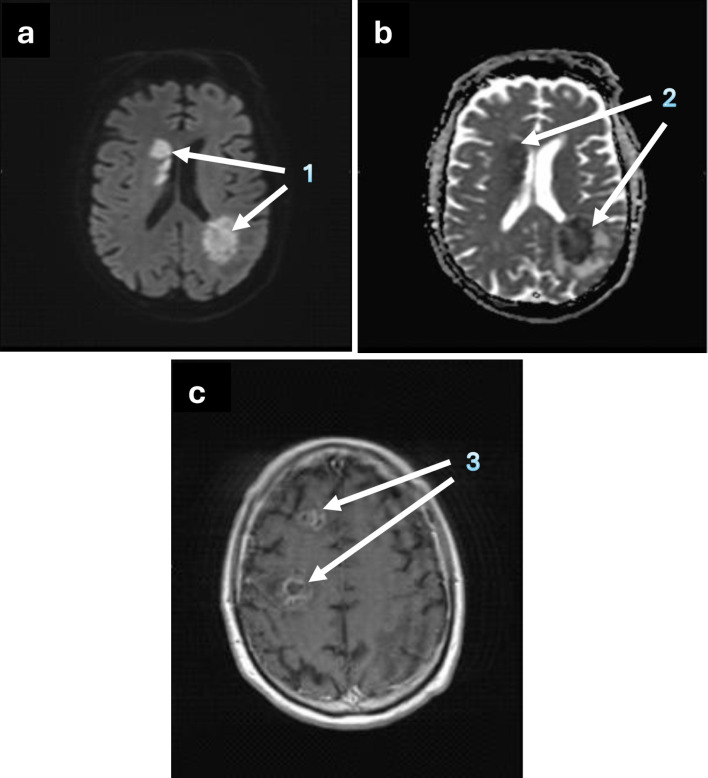
The patient described in this case report was admitted to the San Luigi Hospital in Turin for confusion, drowsiness, and buccal and eye deviation. An acute neurological disease was suspected. He was affected by chronic lymphocytic leukemia (CLL) on active treatment with the novel Bruton tyrosine kinase inhibitor (BTKi) acalabrutinib. Other comorbidities included type II diabetes mellitus, arterial hypertension, and nonalcoholic steatohepatitis. Imaging exams showed multiple brain lesions, which appeared to be of infectious-inflammatory origin. Consequently, therapy with acalabrutinib was withheld. The patient was later transferred to the intensive care unit, because of worsening neurological conditions. The definite diagnosis of fungal abscess was obtained through a stereotactic biopsy of the widest brain lesion. Microbiological tests confirmed Scedosporium spp. as the etiological agent. Once a detailed antibiogram had been obtained, voriconazole therapy was started. However, the patient's clinical conditions decayed rapidly and he later died of neurological complications. BTKis represent a milestone in the treatment of CLL; however, little is known about how these molecules act on the immune system. Fungal brain abscesses are rare conditions more commonly seen in heavily immunocompromised patients, such as those affected by acquired immune deficiency syndrome, after bone marrow transplant or treatment for acute leukemia. Whether or not therapy with BTKis can favor opportunistic fungal infections is still a matter of debate. Various reports of Aspergillosis infections developing after therapy with ibrutinib exist. Evidence does suggest that an iatrogenic impairment in the innate immune system could favor these infections. In addition, the patient's comorbidities, such as diabetes mellitus and advancing hematological disease, might create the ideal breeding ground for these microorganisms.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


