A Real-World Comparison of Drug Trough Levels between Patients Experiencing a Secondary Nonimmune Loss of Response and Those Maintaining a Response to Infliximab on Long-Term Maintenance Therapy for Inflammatory Bowel Disease.
Michael Farber, Jeremy Polman, Nina Kohn, Vincent Chua, Arun Swaminath, Keith Sultan
{"title":"A Real-World Comparison of Drug Trough Levels between Patients Experiencing a Secondary Nonimmune Loss of Response and Those Maintaining a Response to Infliximab on Long-Term Maintenance Therapy for Inflammatory Bowel Disease.","authors":"Michael Farber, Jeremy Polman, Nina Kohn, Vincent Chua, Arun Swaminath, Keith Sultan","doi":"10.1159/000541377","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A secondary loss of response (LOR) to infliximab (IFX) therapy for inflammatory bowel disease (IBD) is typically associated with low IFX trough levels, often with high levels of neutralizing antibodies to IFX (ATI). A small subset of patients on long-term therapy experience a \"nonimmune\" LOR, without ATI and with desired IFX trough levels ≥5 μg/mL, regarded as a LOR to the mechanism of action of IFX. However, this currently accepted IFX goal level is largely derived from observations of patients within the first year of therapy and may not apply to those on treatment beyond 1 year.</p><p><strong>Methods: </strong>Retrospective review of all IBD patients receiving IFX infusions for ≥12 months with at least 1 IFX trough and ATI measurement beyond 12 months was conducted. Chart review of all patients with absent ATI and an IFX trough ≥5 μg/mL classifies as LOR versus non-LOR based on physician assessment, with a comparison of IFX troughs between the two groups.</p><p><strong>Results: </strong>Of 167 patients using IFX ≥12 months, 13 (7.8%) experienced a nonimmune secondary LOR. The mean duration of IFX use was over 3 years for both LOR and non-LOR patients. The mean IFX trough for those with LOR was greater than for those without LOR, 18.5 μg/mL versus 13.1 μg/mL, <i>p</i> = 0.110.</p><p><strong>Conclusion: </strong>Our results did not demonstrate lower IFX levels among patients experiencing secondary nonimmune LOR on long-term therapy. Our results do not redefine the therapeutic IFX goal levels for those patients on long-term therapy and suggest that underdosing of IFX is not the cause of secondary LOR.</p>","PeriodicalId":13605,"journal":{"name":"Inflammatory Intestinal Diseases","volume":"9 1","pages":"252-259"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11521506/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Inflammatory Intestinal Diseases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000541377","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: A secondary loss of response (LOR) to infliximab (IFX) therapy for inflammatory bowel disease (IBD) is typically associated with low IFX trough levels, often with high levels of neutralizing antibodies to IFX (ATI). A small subset of patients on long-term therapy experience a "nonimmune" LOR, without ATI and with desired IFX trough levels ≥5 μg/mL, regarded as a LOR to the mechanism of action of IFX. However, this currently accepted IFX goal level is largely derived from observations of patients within the first year of therapy and may not apply to those on treatment beyond 1 year.
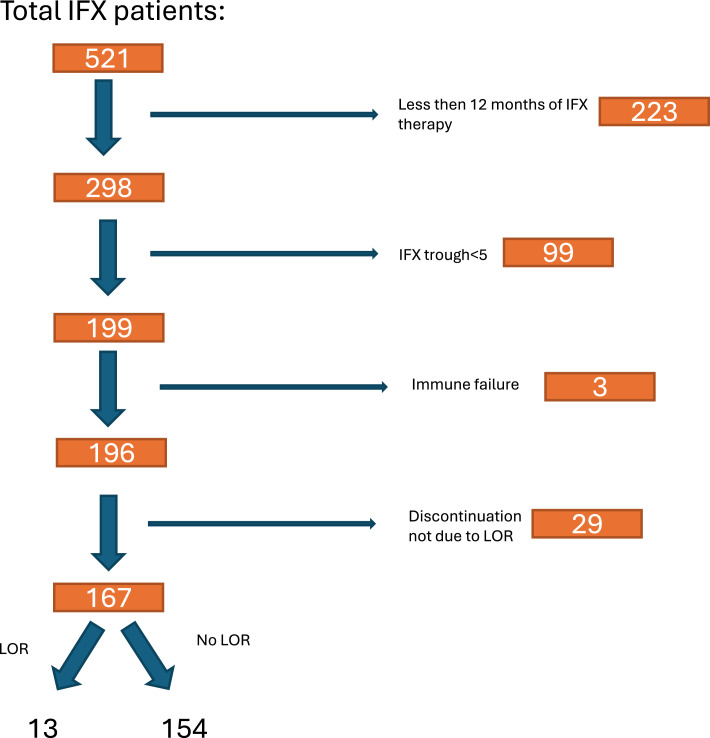
Methods: Retrospective review of all IBD patients receiving IFX infusions for ≥12 months with at least 1 IFX trough and ATI measurement beyond 12 months was conducted. Chart review of all patients with absent ATI and an IFX trough ≥5 μg/mL classifies as LOR versus non-LOR based on physician assessment, with a comparison of IFX troughs between the two groups.
Results: Of 167 patients using IFX ≥12 months, 13 (7.8%) experienced a nonimmune secondary LOR. The mean duration of IFX use was over 3 years for both LOR and non-LOR patients. The mean IFX trough for those with LOR was greater than for those without LOR, 18.5 μg/mL versus 13.1 μg/mL, p = 0.110.
Conclusion: Our results did not demonstrate lower IFX levels among patients experiencing secondary nonimmune LOR on long-term therapy. Our results do not redefine the therapeutic IFX goal levels for those patients on long-term therapy and suggest that underdosing of IFX is not the cause of secondary LOR.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


