Francesco Roscio, Eleonora Monti, Federico Clerici, Francesco Maria Carrano, Ildo Scandroglio
{"title":"Improving outcomes in laparoscopic anterior rectal resection: The benefits of REAL score in preoperative risk assessment for anastomotic leak","authors":"Francesco Roscio, Eleonora Monti, Federico Clerici, Francesco Maria Carrano, Ildo Scandroglio","doi":"10.1016/j.soda.2024.100151","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>The aim of the study is to evaluate the effectiveness of REctal Anastomotic Leak (REAL) score for predicting the risk of anastomotic leakage in patients undergoing laparoscopic anterior rectal resection with total mesorectal excision (lapARR-TME) for rectal cancer.</div></div><div><h3>Methods</h3><div>This prospective study collected data on patients' medical history, surgery, hospital stay, and short-term outcome. We calculated the REAL score for each patient and statistically compared those who experienced an anastomotic leak to those who did not. Additionally, we conducted a univariate and multivariate analysis on other factors that may have influenced outcomes.</div></div><div><h3>Results</h3><div>The study included 57 patients with a mean age of 70 years and a Charlson Comorbidity Index of 6.1 ± 1.9. 57.9% of patients had a loop ileostomy fashioned and Indocyanine green (ICG) angiography was used during surgery in 53.3% of cases. There were 6 cases of anastomotic leakage, with 4 treated surgically and 2 conservatively. Patients with anastomotic leak had a significantly higher REAL score than those without (71.3 ± 20.5 vs. 33.7 ± 21.3). The 30-day readmission and mortality rates were 5.3% and 0%, respectively. Low preoperative serum albumin levels, preoperative blood transfusions, and the absence of ICG angiography during surgery were factors significantly associated with an increased risk of anastomotic leakage according to both univariate and multivariate analyses.</div></div><div><h3>Conclusions</h3><div>The REAL score may be a helpful tool for evaluating the risk of anastomotic leak in patients undergoing lapARR-TME. Further investigation is needed to evaluate the incorporation of additional modifiable factors such as hypoalbuminemia, preoperative transfusion rate, and the use of ICG angiography during surgery.</div></div>","PeriodicalId":101190,"journal":{"name":"Surgery Open Digestive Advance","volume":"16 ","pages":"Article 100151"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Open Digestive Advance","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667008924000259","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background
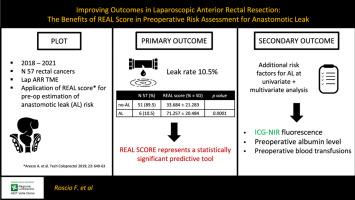
The aim of the study is to evaluate the effectiveness of REctal Anastomotic Leak (REAL) score for predicting the risk of anastomotic leakage in patients undergoing laparoscopic anterior rectal resection with total mesorectal excision (lapARR-TME) for rectal cancer.
Methods
This prospective study collected data on patients' medical history, surgery, hospital stay, and short-term outcome. We calculated the REAL score for each patient and statistically compared those who experienced an anastomotic leak to those who did not. Additionally, we conducted a univariate and multivariate analysis on other factors that may have influenced outcomes.
Results
The study included 57 patients with a mean age of 70 years and a Charlson Comorbidity Index of 6.1 ± 1.9. 57.9% of patients had a loop ileostomy fashioned and Indocyanine green (ICG) angiography was used during surgery in 53.3% of cases. There were 6 cases of anastomotic leakage, with 4 treated surgically and 2 conservatively. Patients with anastomotic leak had a significantly higher REAL score than those without (71.3 ± 20.5 vs. 33.7 ± 21.3). The 30-day readmission and mortality rates were 5.3% and 0%, respectively. Low preoperative serum albumin levels, preoperative blood transfusions, and the absence of ICG angiography during surgery were factors significantly associated with an increased risk of anastomotic leakage according to both univariate and multivariate analyses.
Conclusions
The REAL score may be a helpful tool for evaluating the risk of anastomotic leak in patients undergoing lapARR-TME. Further investigation is needed to evaluate the incorporation of additional modifiable factors such as hypoalbuminemia, preoperative transfusion rate, and the use of ICG angiography during surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


