Evaluating the relationship between glycemic control and bone fragility within the UK Biobank: observational and one-sample Mendelian randomization analyses.
Samuel Ghatan, Fjorda Koromani, Katerina Trajanoska, Evert F S van Velsen, Maryam Kavousi, M Carola Zillikens, Carolina Medina-Gomez, Ling Oei, Fernando Rivadeneira
{"title":"Evaluating the relationship between glycemic control and bone fragility within the UK Biobank: observational and one-sample Mendelian randomization analyses.","authors":"Samuel Ghatan, Fjorda Koromani, Katerina Trajanoska, Evert F S van Velsen, Maryam Kavousi, M Carola Zillikens, Carolina Medina-Gomez, Ling Oei, Fernando Rivadeneira","doi":"10.1093/jbmrpl/ziae126","DOIUrl":null,"url":null,"abstract":"<p><p>We aimed to: (1) examine the relationship between glycemic control, BMD estimated from heel ultrasound (eBMD) and fracture risk in individuals with type 1 (T1D) and type 2 diabetes (T2D) and (2) perform a one-sample Mendelian randomization (MR) study to explore potential causal associations between glycemic control, eBMD, and fractures. This study comprised 452 131 individuals from the UK Biobank with glycated hemoglobin A1C (HbA<sub>1c</sub>) and eBMD levels. At baseline, 4078 participants were diagnosed with T1D and 23 682 with T2D. HbA<sub>1c</sub> was used to classify patients into \"adequately-\" (ACD; <i>n</i> = 17 078; HbA<sub>1c</sub> < 7.0%/53 mmol/mol) and \"inadequately-\" (ICD; <i>n</i> = 10 682; HbA<sub>1c</sub> ≥ 7.0%/53 mmol/mol) controlled diabetes. In individuals with T1D, a 1% unit (11 mmol/mol) increase in HbA<sub>1c</sub> levels was associated with a 12% increase in fracture risk (HR: 1.12, 95% CI [1.05-1.19]). Fracture risk was highest in individuals with T1D and ICD (HR 2.84, 95%CI [2.53, 3.19]), followed by those with ACD (HR 2.26, 95%CI [1.91, 2.69]), as compared to subjects without diabetes. Evidence for a non-linear association between HbA<sub>1c</sub> and fracture risk was observed (F-test ANOVA <i>p</i>-value = 0.002) in individuals with T2D, with risk being increased at both low and high levels of HbA<sub>1c</sub>. Fracture risk between the T2D ACD and ICD groups was not significantly different (HR: 0.97, 95%CI [0.91-1.16]), despite increased BMD. In MR analyses genetically predicted higher HbA<sub>1c</sub> levels were not significantly associated with fracture risk (causal risk ratio: 1.04, 95%CI [0.95-1.14]). We did observe evidence of a non-linear causal association with eBMD (quadratic test <i>p</i>-value = 0.0002), indicating U-shaped relationship between HbA<sub>1c</sub> and eBMD. We obtained evidence that lower HbA<sub>1c</sub> levels will reduce fracture risk in patients with T1D. In individuals with T2D, lowering HbA<sub>1c</sub> levels can mitigate the risk of fractures up to a threshold, beyond which the risk may begin to rise again.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 11","pages":"ziae126"},"PeriodicalIF":2.4000,"publicationDate":"2024-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515132/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
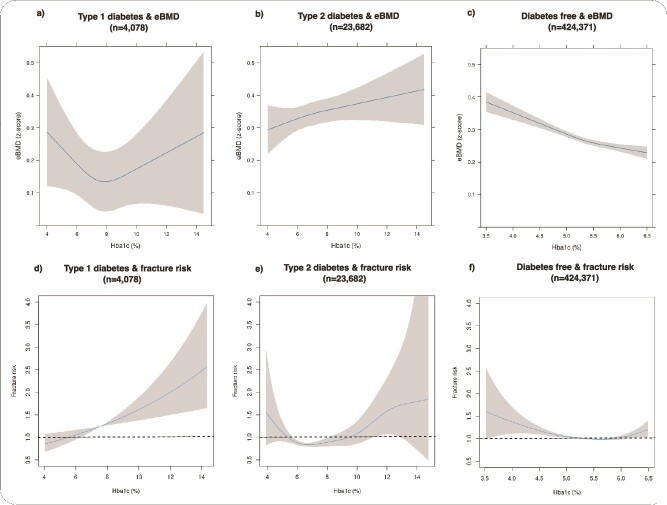
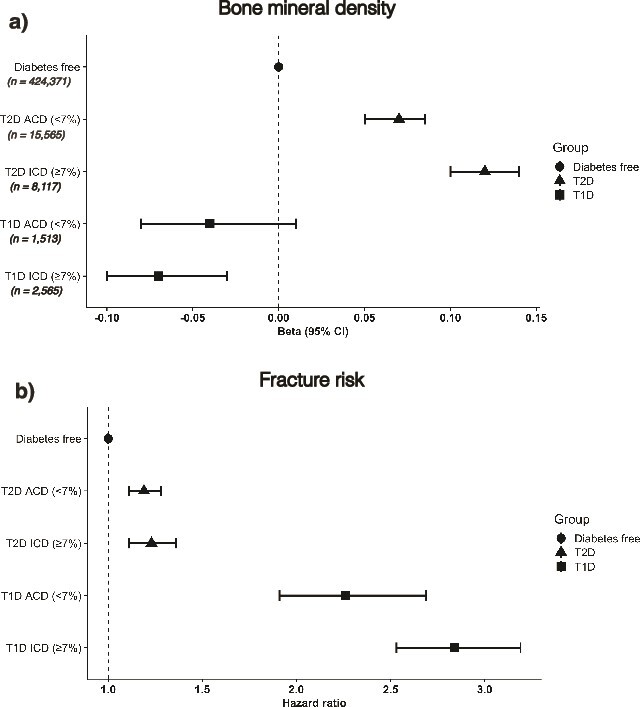
We aimed to: (1) examine the relationship between glycemic control, BMD estimated from heel ultrasound (eBMD) and fracture risk in individuals with type 1 (T1D) and type 2 diabetes (T2D) and (2) perform a one-sample Mendelian randomization (MR) study to explore potential causal associations between glycemic control, eBMD, and fractures. This study comprised 452 131 individuals from the UK Biobank with glycated hemoglobin A1C (HbA1c) and eBMD levels. At baseline, 4078 participants were diagnosed with T1D and 23 682 with T2D. HbA1c was used to classify patients into "adequately-" (ACD; n = 17 078; HbA1c < 7.0%/53 mmol/mol) and "inadequately-" (ICD; n = 10 682; HbA1c ≥ 7.0%/53 mmol/mol) controlled diabetes. In individuals with T1D, a 1% unit (11 mmol/mol) increase in HbA1c levels was associated with a 12% increase in fracture risk (HR: 1.12, 95% CI [1.05-1.19]). Fracture risk was highest in individuals with T1D and ICD (HR 2.84, 95%CI [2.53, 3.19]), followed by those with ACD (HR 2.26, 95%CI [1.91, 2.69]), as compared to subjects without diabetes. Evidence for a non-linear association between HbA1c and fracture risk was observed (F-test ANOVA p-value = 0.002) in individuals with T2D, with risk being increased at both low and high levels of HbA1c. Fracture risk between the T2D ACD and ICD groups was not significantly different (HR: 0.97, 95%CI [0.91-1.16]), despite increased BMD. In MR analyses genetically predicted higher HbA1c levels were not significantly associated with fracture risk (causal risk ratio: 1.04, 95%CI [0.95-1.14]). We did observe evidence of a non-linear causal association with eBMD (quadratic test p-value = 0.0002), indicating U-shaped relationship between HbA1c and eBMD. We obtained evidence that lower HbA1c levels will reduce fracture risk in patients with T1D. In individuals with T2D, lowering HbA1c levels can mitigate the risk of fractures up to a threshold, beyond which the risk may begin to rise again.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


