Oliver J Watkeys, Kimberlie Dean, Kristin R Laurens, Vaughan J Carr, Melissa J Green
{"title":"Medicare-subsidised mental health service use during the first 15 years of life in New South Wales: a population cohort study","authors":"Oliver J Watkeys, Kimberlie Dean, Kristin R Laurens, Vaughan J Carr, Melissa J Green","doi":"10.5694/mja2.52498","DOIUrl":null,"url":null,"abstract":"<p>Each year, one in seven Australian children and adolescents experience a mental disorder, but only half receive treatment.<span><sup>1</sup></span> The Australian Institute of Health and Welfare (AIHW) reported that 6% of children aged 5–11 years and 13% of those aged 12–17 years used Medicare-subsidised mental health services during 2021–22.<span><sup>2</sup></span></p><p>We investigated the annual and cumulative incidence of Medicare-subsidised mental health services for children during their first 15 years of life, and the demographic characteristics associated with the types of services used. We analysed Medicare Benefits Schedule (MBS) data for 86 759 children born during 1 January 2002 – 31 December 2005 and included in the New South Wales Child Development Study,<span><sup>3</sup></span> or 94.7% of the record linkage cohort; 4848 children were excluded because information for socio-demographic indices were not recorded in the 2009 NSW Australian Early Development Census.<span><sup>4</sup></span> Record linkage was performed by the NSW Centre for Health Record Linkage (CHeReL) and the AIHW Data Integration Services Centre.</p><p>MBS records for mental health services (1 January 2002 – 31 December 2018) were categorised as being delivered by general practitioners (Better Access treatment plans), psychologists, psychiatrists, occupational therapists or social workers, or other (group therapy, psychological services provided by general practitioners or paediatricians) (Supporting Information, table 1). We assessed associations between demographic factors — sex, Indigenous status, socio-economic position (Index of Relative Socioeconomic Disadvantage),<span><sup>5</sup></span> geographic remoteness (Accessibility/Remoteness Index of Australia)<span><sup>6</sup></span> — and each MBS-subsidised mental health service type in univariable and multivariable logistic regression analyses; we report odds ratios with 99.924% confidence intervals (Bonferroni-adjusted for multiple testing). The NSW Population and Health Services Research Ethics Committee and ACT Health Human Research Ethics Committee (HREC/18/ciphs/49) and the Australian Institute of Health and Welfare Ethics Committee (EO2020/4/1026) approved the study. We report the study in accordance with the STROBE reporting guidelines for observational studies.<span><sup>7</sup></span></p><p>A total of 23 330 of 86 759 children (26.9%) had used MBS-subsidised mental health services prior to their 15th birthdays: 21 535 had received Better Access plans (24.8%), 15 693 had received care from psychologists (18.1%), 2306 had consulted psychiatrists (2.7%), 1844 had received psychological therapy from occupational therapists or social workers (2.1%), and 2391 had received other mental health service types (2.8%) (Box 1). The annual and cumulative incidence of mental health service use each increased exponentially with age for Better Access plans and psychologist care, and more gradually for care from other mental health service providers (Box 2). Boys were more likely than girls to receive mental health services from occupational therapists or social workers or from other sources, and less likely to receive Better Access plans. Indigenous children and children living in postcodes of lower socio-economic disadvantage were more likely to use any mental health service, including Better Access plans, psychologist care, and psychiatrist care. Children in inner regional areas were more likely than those in major cities to receive any mental health treatment, including Better Access plans, psychologist care, and services from occupational therapists or social workers; children in outer regional, remote, or very remote areas were less likely than children in major cities to use mental health services (any, Better Access plans, psychologist care). The likelihood of mental health service use by data follow-up (31 December 2018) increased with age (Box 3).</p><p>We found that 26.9% of children had used Medicare-subsidised mental health services before their 15th birthdays, a proportion considerably larger than the annual incidence at age 14 years (10.5%) or that reported in an earlier AIHW publication.<span><sup>2</sup></span> The likelihood of mental health service use was lower among non-Indigenous than Indigenous children and among children in socio-economically disadvantaged or outer regional or remote areas, consistent with other reports.<span><sup>8, 9</sup></span> Girls were more likely than boys to receive Better Access plans, but boys were more likely to receive care from occupational therapists or social workers and use “other” mental health service types, possibly because of earlier detection of externalising disorders, which are more prevalent among boys.<span><sup>10</sup></span> Service use was greater for children older at the time of follow-up, probably because of the higher incidence of mental disorders during adolescence than earlier in life.<span><sup>2, 10</sup></span> The primary limitations of our study were the unavailability of data for mental health care not covered by MBS data (eg, Headspace, privately funded, hospital and emergency, and school-based care) and the fact that we could not adjust our analyses for repeat presentations by individual children. Additional work is needed to ensure equitable access to mental health services for all young people in Australia.</p><p>The data used in this study have been provided by government custodians for research purposes of the NSW Child Development Study and cannot be shared with third parties or deposited in data repositories. Researchers wishing to access these data need to apply in writing to the relevant data custodians.</p><p>No relevant disclosures.</p>","PeriodicalId":18214,"journal":{"name":"Medical Journal of Australia","volume":"221 10","pages":"554-557"},"PeriodicalIF":6.7000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.5694/mja2.52498","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Journal of Australia","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.5694/mja2.52498","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Each year, one in seven Australian children and adolescents experience a mental disorder, but only half receive treatment.1 The Australian Institute of Health and Welfare (AIHW) reported that 6% of children aged 5–11 years and 13% of those aged 12–17 years used Medicare-subsidised mental health services during 2021–22.2
We investigated the annual and cumulative incidence of Medicare-subsidised mental health services for children during their first 15 years of life, and the demographic characteristics associated with the types of services used. We analysed Medicare Benefits Schedule (MBS) data for 86 759 children born during 1 January 2002 – 31 December 2005 and included in the New South Wales Child Development Study,3 or 94.7% of the record linkage cohort; 4848 children were excluded because information for socio-demographic indices were not recorded in the 2009 NSW Australian Early Development Census.4 Record linkage was performed by the NSW Centre for Health Record Linkage (CHeReL) and the AIHW Data Integration Services Centre.
MBS records for mental health services (1 January 2002 – 31 December 2018) were categorised as being delivered by general practitioners (Better Access treatment plans), psychologists, psychiatrists, occupational therapists or social workers, or other (group therapy, psychological services provided by general practitioners or paediatricians) (Supporting Information, table 1). We assessed associations between demographic factors — sex, Indigenous status, socio-economic position (Index of Relative Socioeconomic Disadvantage),5 geographic remoteness (Accessibility/Remoteness Index of Australia)6 — and each MBS-subsidised mental health service type in univariable and multivariable logistic regression analyses; we report odds ratios with 99.924% confidence intervals (Bonferroni-adjusted for multiple testing). The NSW Population and Health Services Research Ethics Committee and ACT Health Human Research Ethics Committee (HREC/18/ciphs/49) and the Australian Institute of Health and Welfare Ethics Committee (EO2020/4/1026) approved the study. We report the study in accordance with the STROBE reporting guidelines for observational studies.7
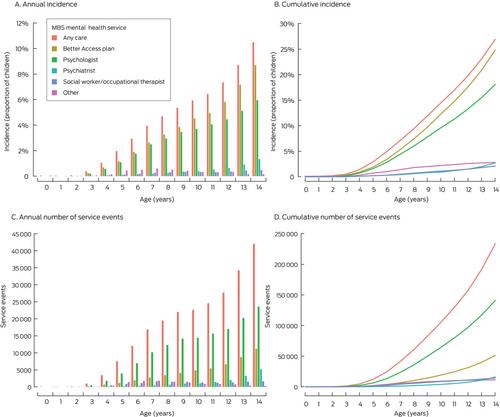
A total of 23 330 of 86 759 children (26.9%) had used MBS-subsidised mental health services prior to their 15th birthdays: 21 535 had received Better Access plans (24.8%), 15 693 had received care from psychologists (18.1%), 2306 had consulted psychiatrists (2.7%), 1844 had received psychological therapy from occupational therapists or social workers (2.1%), and 2391 had received other mental health service types (2.8%) (Box 1). The annual and cumulative incidence of mental health service use each increased exponentially with age for Better Access plans and psychologist care, and more gradually for care from other mental health service providers (Box 2). Boys were more likely than girls to receive mental health services from occupational therapists or social workers or from other sources, and less likely to receive Better Access plans. Indigenous children and children living in postcodes of lower socio-economic disadvantage were more likely to use any mental health service, including Better Access plans, psychologist care, and psychiatrist care. Children in inner regional areas were more likely than those in major cities to receive any mental health treatment, including Better Access plans, psychologist care, and services from occupational therapists or social workers; children in outer regional, remote, or very remote areas were less likely than children in major cities to use mental health services (any, Better Access plans, psychologist care). The likelihood of mental health service use by data follow-up (31 December 2018) increased with age (Box 3).
We found that 26.9% of children had used Medicare-subsidised mental health services before their 15th birthdays, a proportion considerably larger than the annual incidence at age 14 years (10.5%) or that reported in an earlier AIHW publication.2 The likelihood of mental health service use was lower among non-Indigenous than Indigenous children and among children in socio-economically disadvantaged or outer regional or remote areas, consistent with other reports.8, 9 Girls were more likely than boys to receive Better Access plans, but boys were more likely to receive care from occupational therapists or social workers and use “other” mental health service types, possibly because of earlier detection of externalising disorders, which are more prevalent among boys.10 Service use was greater for children older at the time of follow-up, probably because of the higher incidence of mental disorders during adolescence than earlier in life.2, 10 The primary limitations of our study were the unavailability of data for mental health care not covered by MBS data (eg, Headspace, privately funded, hospital and emergency, and school-based care) and the fact that we could not adjust our analyses for repeat presentations by individual children. Additional work is needed to ensure equitable access to mental health services for all young people in Australia.
The data used in this study have been provided by government custodians for research purposes of the NSW Child Development Study and cannot be shared with third parties or deposited in data repositories. Researchers wishing to access these data need to apply in writing to the relevant data custodians.
期刊介绍:
The Medical Journal of Australia (MJA) stands as Australia's foremost general medical journal, leading the dissemination of high-quality research and commentary to shape health policy and influence medical practices within the country. Under the leadership of Professor Virginia Barbour, the expert editorial team at MJA is dedicated to providing authors with a constructive and collaborative peer-review and publication process. Established in 1914, the MJA has evolved into a modern journal that upholds its founding values, maintaining a commitment to supporting the medical profession by delivering high-quality and pertinent information essential to medical practice.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


