Elizaveta Bokova, Shimon E Jacobs, Laura Tiusaba, Christina P Ho, Briony K Varda, Hans G Pohl, Christina Feng, Victoria A Lane, Caitlin A Smith, Andrea T Badillo, Richard J Wood, Marc A Levitt
{"title":"A Modification of the Newborn Operation for Cloacal Exstrophy: Leaving the Cecal Plate Untouched.","authors":"Elizaveta Bokova, Shimon E Jacobs, Laura Tiusaba, Christina P Ho, Briony K Varda, Hans G Pohl, Christina Feng, Victoria A Lane, Caitlin A Smith, Andrea T Badillo, Richard J Wood, Marc A Levitt","doi":"10.1055/s-0044-1791814","DOIUrl":null,"url":null,"abstract":"<p><p>The conventional approach to managing a newborn with cloacal exstrophy typically includes separating the cecal plate from between the two hemibladders, tubularizing it to be included in the fecal stream, creating an end colostomy, and bringing the two bladder halves together. This study introduces an alternative approach wherein the cecal plate is retained in its original position and designated for future use as an autoaugment of the bladder. Four cases of cloacal exstrophy cases managed between November 2019 and February 2024 are described, with surgical approach and postoperative outcomes reported. Two patients who underwent traditional reconstruction experienced bacterial overgrowth attributed to stasis in the cecal plate, which manifested in increased ostomy output and feeding intolerance. Treatment in these two cases was to remove the cecum from the fecal stream and use it instead for a bladder augment. Learning from these cases, the third and fourth newborn's approach involved retaining the cecum in situ for autoaugmentation of the bladder and performing an ileal to hindgut anastomosis. No postoperative acidosis occurred in these patients. The alternative approach to the newborn management of cloacal exstrophy whereby the cecal plate is left in situ can decrease stasis and postoperative bacterial overgrowth. It allows for an autoaugmentation of the bladder and is technically easier than the traditional rescue of the cecal plate from within the two hemibladders.</p>","PeriodicalId":43204,"journal":{"name":"European Journal of Pediatric Surgery Reports","volume":"12 1","pages":"e63-e67"},"PeriodicalIF":0.7000,"publicationDate":"2024-10-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11493485/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Pediatric Surgery Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0044-1791814","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
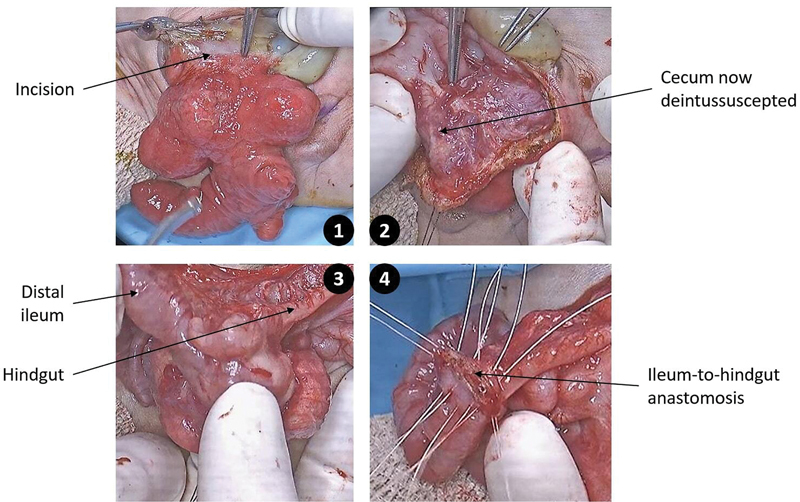
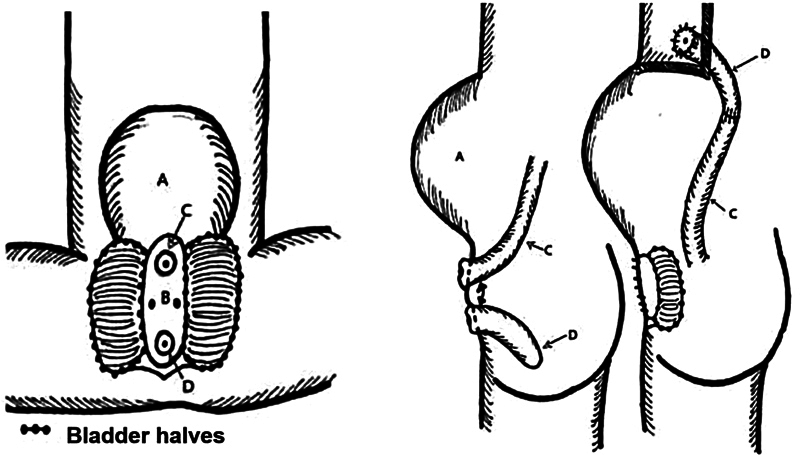
The conventional approach to managing a newborn with cloacal exstrophy typically includes separating the cecal plate from between the two hemibladders, tubularizing it to be included in the fecal stream, creating an end colostomy, and bringing the two bladder halves together. This study introduces an alternative approach wherein the cecal plate is retained in its original position and designated for future use as an autoaugment of the bladder. Four cases of cloacal exstrophy cases managed between November 2019 and February 2024 are described, with surgical approach and postoperative outcomes reported. Two patients who underwent traditional reconstruction experienced bacterial overgrowth attributed to stasis in the cecal plate, which manifested in increased ostomy output and feeding intolerance. Treatment in these two cases was to remove the cecum from the fecal stream and use it instead for a bladder augment. Learning from these cases, the third and fourth newborn's approach involved retaining the cecum in situ for autoaugmentation of the bladder and performing an ileal to hindgut anastomosis. No postoperative acidosis occurred in these patients. The alternative approach to the newborn management of cloacal exstrophy whereby the cecal plate is left in situ can decrease stasis and postoperative bacterial overgrowth. It allows for an autoaugmentation of the bladder and is technically easier than the traditional rescue of the cecal plate from within the two hemibladders.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


