Video head impulse gain is impaired in myotonic dystrophy types 1 and 2
Abstract
Background and Purpose
This study was undertaken to examine vestibulo-ocular reflex (VOR) characteristics in myotonic dystrophy type 1 (DM1) and type 2 (DM2) using video head impulse testing (vHIT).
Methods
VOR gain, refixation saccade prevalence, first saccade amplitude, onset latency, peak velocity, and duration were compared in DM1, DM2, age-matched normal controls, and patients with peripheral and central vestibulopathies.
Results
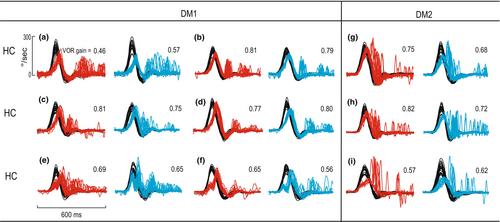
Fifty percent of DM1 and 37.5% of DM2 patients demonstrated reduced VOR gain. Refixation saccade prevalence for horizontal canal (HC) and posterior canal (PC) was significantly higher in DM1 (101 ± 42%, 82 ± 47%) and DM2 (70 ± 45%, 61 ± 38%) compared to controls (40 ± 28% and 43 ± 33%, p < 0.05). The first saccade amplitudes and peak velocities were higher in HC and PC planes in DM1 and DM2 compared to controls (p < 0.05). HC slow phase eye velocity profiles in DM1 showed delayed peaks. The asymmetry ratio, which represents the percentage difference between the first and second halves of the slow phase eye velocity response, was therefore negative (−22.5 ± 17%, −2.3 ± 16%, and − 4.7 ± 8% in DM1, DM2, and controls). HC VOR gains were lower and gain asymmetry ratio was larger and negative in patients with DM1 with moderate to severe ptosis and a history of imbalance and falls compared to the remaining DM1 patients (p < 0.05). In peripheral vestibulopathies, saccade amplitude was larger, peak velocity was higher, and onset latency was shorter (p < 0.05) than in DM1. In central vestibulopathy (posterior circulation strokes), saccade peak velocity was higher, but amplitude and onset latency were not significantly different from DM1.
Conclusions
VOR impairment is common in DM1 and DM2. In DM1, refixation saccade characteristics are closer to central than peripheral vestibulopathies. Delayed peaks in the vHIT eye velocity profile observed in patients with DM1 may reflect extraocular muscle weakness. VOR impairment and VOR asymmetry in DM1 are associated with imbalance and falls.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


