{"title":"Influence of a surgeon's exposure to operating room turnover delays on patient outcomes.","authors":"Arnaud Pasquer, Quentin Cordier, Jean-Christophe Lifante, Gilles Poncet, Stéphanie Polazzi, Antoine Duclos","doi":"10.1093/bjsopen/zrae117","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A surgeon's daily performance may be affected by operating room organizational factors, potentially impacting patient outcomes. The aim of this study was to investigate the link between a surgeon's exposure to delays in starting scheduled operations and patient outcomes.</p><p><strong>Methods: </strong>A prospective observational study was conducted from 1 November 2020 to 31 December 2021, across 14 surgical departments in four university hospitals, covering various surgical disciplines. All elective surgeries by 45 attending surgeons were analysed, assessing delays in starting operations and inter-procedural wait times exceeding 1 or 2 h. The primary outcome was major adverse events within 30 days post-surgery. Mixed-effect logistic regression accounted for operation clustering within surgeons, estimating adjusted relative risks and outcome rate differences using marginal standardization.</p><p><strong>Results: </strong>Among 8844 elective operations, 4.0% started more than 1 h late, associated with an increased rate of adverse events (21.6% versus 14.4%, P = 0.039). Waiting time surpassing 1 h between procedures occurred in 71.4% of operations and was also associated with a higher frequency of adverse events (13.9% versus 5.3%, P < 0.001). After adjustment, delayed operations were associated with an elevated risk of major adverse events (adjusted relative risk 1.37 (95% c.i. 1.06 to 1.85)). The standardized rate of major adverse events was 12.1%, compared with 8.9% (absolute difference of 3.3% (95% c.i. 0.6% to 5.6%)), when a surgeon experienced a delay in operating room scheduling or waiting time between two procedures exceeding 1 h, as opposed to not experiencing such delays.</p><p><strong>Conclusion: </strong>A surgeon's exposure to delay before starting elective procedures was associated with an increased occurrence of major adverse events. Optimizing operating room turnover to prevent delayed operations and waiting time is critical for patient safety.</p>","PeriodicalId":9028,"journal":{"name":"BJS Open","volume":"8 5","pages":""},"PeriodicalIF":4.5000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11477981/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BJS Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/bjsopen/zrae117","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A surgeon's daily performance may be affected by operating room organizational factors, potentially impacting patient outcomes. The aim of this study was to investigate the link between a surgeon's exposure to delays in starting scheduled operations and patient outcomes.
Methods: A prospective observational study was conducted from 1 November 2020 to 31 December 2021, across 14 surgical departments in four university hospitals, covering various surgical disciplines. All elective surgeries by 45 attending surgeons were analysed, assessing delays in starting operations and inter-procedural wait times exceeding 1 or 2 h. The primary outcome was major adverse events within 30 days post-surgery. Mixed-effect logistic regression accounted for operation clustering within surgeons, estimating adjusted relative risks and outcome rate differences using marginal standardization.
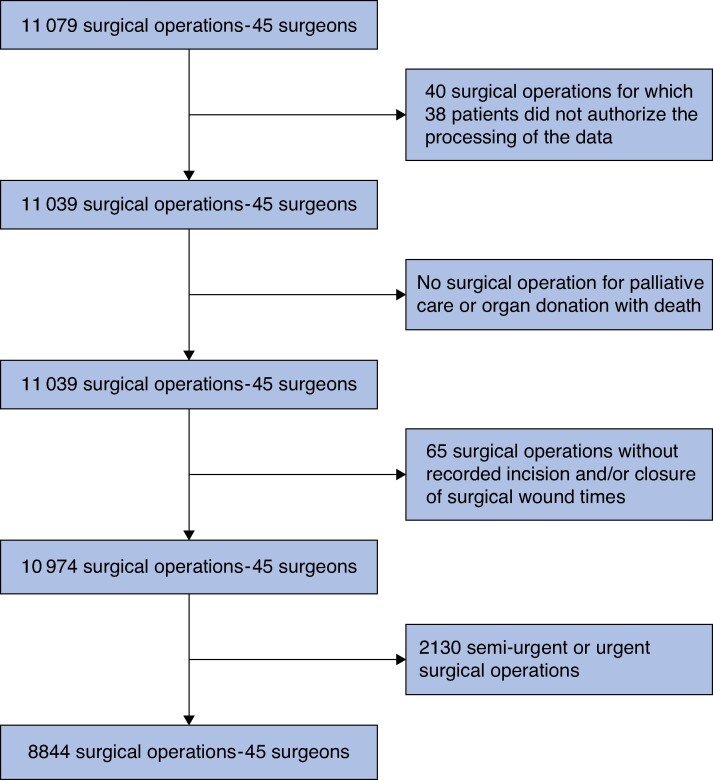
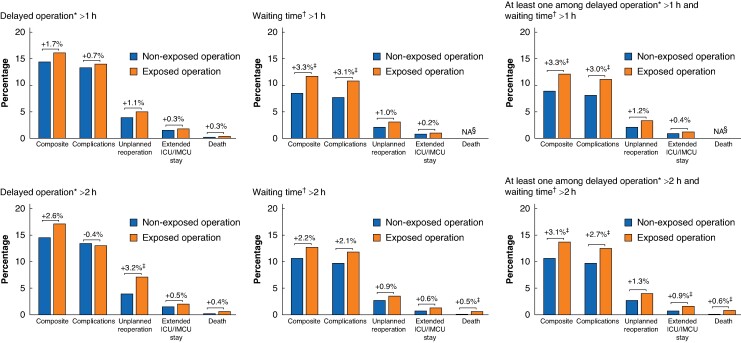
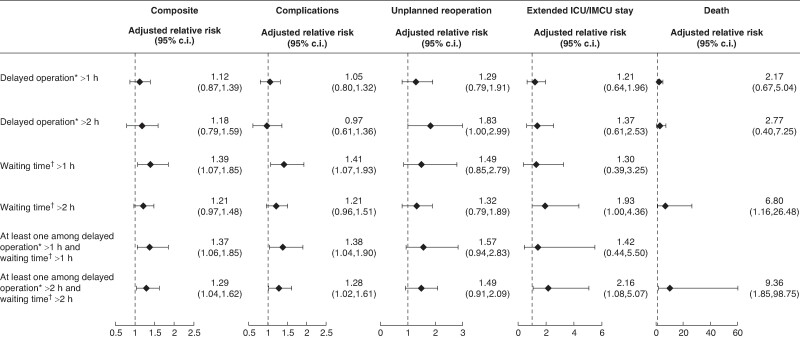
Results: Among 8844 elective operations, 4.0% started more than 1 h late, associated with an increased rate of adverse events (21.6% versus 14.4%, P = 0.039). Waiting time surpassing 1 h between procedures occurred in 71.4% of operations and was also associated with a higher frequency of adverse events (13.9% versus 5.3%, P < 0.001). After adjustment, delayed operations were associated with an elevated risk of major adverse events (adjusted relative risk 1.37 (95% c.i. 1.06 to 1.85)). The standardized rate of major adverse events was 12.1%, compared with 8.9% (absolute difference of 3.3% (95% c.i. 0.6% to 5.6%)), when a surgeon experienced a delay in operating room scheduling or waiting time between two procedures exceeding 1 h, as opposed to not experiencing such delays.
Conclusion: A surgeon's exposure to delay before starting elective procedures was associated with an increased occurrence of major adverse events. Optimizing operating room turnover to prevent delayed operations and waiting time is critical for patient safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


