Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen, Haoyu Bai, Linghua Yan, Li Xiao, Jun You
{"title":"Comprehensive genomic analysis of molecular residual disease based on circulating tumour DNA in postoperative patients with colorectal cancer","authors":"Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen, Haoyu Bai, Linghua Yan, Li Xiao, Jun You","doi":"10.1002/ctm2.70041","DOIUrl":null,"url":null,"abstract":"<p>Dear Editor,</p><p>Colorectal cancer (CRC) is a major global health issue with a 40% 5-year mortality rate,<span><sup>1</sup></span> and 30%−50% of patients still experience recurrence after curative resection.<span><sup>2, 3</sup></span> The clinical utility of molecular residual disease (MRD) detection in risk stratification and recurrence detection using circulating tumour DNA (ctDNA) noninvasively has attracted widespread attention but with limited studies.<span><sup>4-7</sup></span> We measured the value of tumour-agnostic ctDNA-guided MRD for recurrence prediction and monitoring, and explored the biological characteristics of ctDNA from MRD.</p><p>We included 104 patients with stage I-IV CRC (Figure S1), aged 26 to 82 years. Fourteen (13.5%) patients had positive landmark MRD, and thirty-two (30.8%) patients had positive longitudinal MRD (Table S1). The most frequently variant genes in tumour tissue were <i>TP53</i>, <i>KRAS</i> and <i>APC</i> (Figure S2A), while in ctDNA were <i>KRAS</i>, <i>EGFR</i> and <i>TP53</i> (Figure S2B).</p><p>Patients with negative landmark MRD had a lower recurrence percentage than positive cases (11.1% vs. 57.1%, <i>p</i> < .001), yielding a negative predictive value (NPV) of 88.9% (Figure 1A). The latter group had a significantly higher recurrence risk (hazard ratio [HR], 7.325; <i>p</i> < .001, Figure 1B). As for longitudinal MRD, the recurrence percentage was higher in positive-MRD compared to negative-MRD (43.8% vs. 5.6%, <i>p</i> < .001), yielding a high NPV (94.4%, Figure 1C). Positive longitudinal MRD was correlated with an elevated risk of recurrence (HR: 9.385; <i>p</i> < .001, Figure 1D). In multivariate analysis for disease-free survival (DFS), landmark and longitudinal MRD-positive were significantly associated with increased recurrence risks (Figure 1E). Furthermore, we explored the effect of longitudinal MRD status in patients receiving and not receiving neoadjuvant therapy (NAT). In both groups, longitudinal positive-MRD patients had higher recurrence risk than negative-MRD patients (NAT: HR, 12.509, <i>p</i> = .011; non-NAT: HR, 9.611, <i>p</i> < .001; Figure S3A and B). The recurrence risk was lower in those with negative landmark ctDNA and negative longitudinal ctDNA (Figure S4A–D). Although the NPV for ctDNA was slightly higher than that for MRD, the PPV for ctDNA was lower than that for MRD. The area under the curve (AUC) of 3-year DFS for landmark MRD was .678, longitudinal MRD was .895, and landmark and longitudinal MRD had higher AUCs than ctDNA (Figure S4E). Fourteen out of 18 cases with recurrence detected MRD at the postoperative time points (Figure 1F). And 85.7% (12/14) patients had positive MRD detection before computed tomography confirmed recurrence (median: 198.5 days, Figure 1G). For MRD-positive cases, actions such as initiating adjuvant therapies, more aggressive treatment, intensified monitoring, or early intervention before clinical relapse occurs, may be clinically undertaken, potentially leading to better disease control, improved survival rates, and enhanced quality of life.</p><p>Genetic markers showed complex interactions with clinical outcomes. <i>KRAS</i>, <i>APC</i>, <i>FGFR2</i> and <i>RET</i> variants in ctDNA were associated with inferior DFS (Figure 2A–D). In tissue, <i>KRAS</i> and <i>PIK3CA</i> variants may have the prediction potential for DFS (both <i>p</i> > .05, Figure 2E and F). The recurrence percentage in patients with <i>KRAS</i> variants in cell-free DNA (cfDNA_<i>KRAS+</i>) was significantly higher than those without (Figure 2G). Patients at an earlier stage exhibited a significantly better DFS (Figure S5). In the negative landmark MRD group, patients with metastases had higher variant frequencies of <i>KRAS</i>, <i>ALK</i>, <i>RET</i> and <i>NTRK2</i> than those without (Table S2). A similar trend for these genes was observed in longitudinal MRD-negative patients (Table S3). The tumour mutation burden did not exhibit predictive capability for DFS, while the patients with high microsatellite instability tended to have a better DFS (Figure 2H and I).</p><p>The combination of MRD status with cfDNA_<i>KRAS+</i> was significantly associated with patients’ outcomes. Among patients with positive landmark MRD and positive longitudinal MRD, cfDNA_<i>KRAS+</i> showed a trend to poorer DFS (Figure 3A and B). In patients with negative landmark MRD, cfDNA_<i>KRAS+</i> was associated with poorer DFS (Figure 3A). Then, patients with a positive result in at least one of the 2 statuses (cfDNA_<i>KRAS</i> variants and MRD) were designated as positive. The combination of landmark MRD and cfDNA_<i>KRAS+</i>, and the combination of longitudinal MRD and cfDNA_<i>KRAS+</i> were significantly associated with inferior DFS (Figure 3C and D). For the 3-year DFS, the combination of landmark MRD and cfDNA_<i>KRAS+</i> reached an AUC of .768, surpassing both landmark MRD (.678) and cfDNA_<i>KRAS+</i> (.681). Similarly, the integration of longitudinal MRD and cfDNA_<i>KRAS+</i> reached an AUC of .922, surpassing both longitudinal MRD (.895) and cfDNA_<i>KRAS+</i> (.681) (Figure 3E).</p><p>The recurrence risk of MRD-positive and MRD-negative patients stratified by the adjuvant therapy (AT) was analysed. No survival benefit was observed from AT in landmark MRD-positive patients due to the limited number of patients without AT (<i>n</i> = 2; Figure S6A and C). Patients with AT tended to have shorter DFS and higher percentage of recurrence than patients without AT in the landmark MRD-negative group (Figure S6B and D). Adjuvant therapy may not be suitable for landmark MRD-negative CRC patients to prevent over-medicalisation.</p><p>The I/II class mutation sites and all mutation sites were predominantly concentrated in fragments below 200 bp (Figure 4A and E). Furthermore, we compared the proportion of mutation reads at different length intervals. The proportions of class I/II mutation reads and all mutation reads in the fragments ≤ 100 bp were significantly higher than those in the fragments >100 bp (Figure 4B and F). The percentages of fragments ≤ 100 bp in class I/II mutation reads and all mutation reads were higher than those in non-mutated reads (Figure 4C and G). The median length of class I/II mutation reads was lower than non-mutated reads (163 bp vs. 168 bp; Figure 4D). The median length of all mutation reads was also lower (166 bp vs. 169 bp; Figure 4H). Mutation sites were enriched in shorter fragments, which could potentially improve cfDNA detection methods, guiding the risk stratification, prognostic prediction, and monitoring of disease recurrence.</p><p>Our research underscored the remarkable prognostic value of ctDNA-based MRD monitoring in postoperative CRC patients. Notably, integrating cfDNA_KRAS variants with MRD significantly enhanced the precision of risk stratification. Furthermore, our findings revealed a trend towards enriching mutation sites within shorter cfDNA fragments, offering pivotal insights for developing advanced cfDNA detection strategies.</p><p>Jun You, Li Xiao and Linghua Yan conceived of the study plan. Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen, Haoyu Bai and Linghua Yan collected, analysed and interpreted data. Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen and Haoyu Bai drafted the manuscript. Jun You, Li Xiao and Linghua Yan revised the manuscript. All authors reviewed the manuscript and had final approval of the submitted and published version.</p><p>The authors have no conflict of interest to declare.</p><p>This study was approved by the ethics committee of the corresponding hospital, and was carried out in compliance with the Declaration of Helsinki Principles. Written informed consent was obtained from all study participants.</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"14 10","pages":""},"PeriodicalIF":7.9000,"publicationDate":"2024-10-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ctm2.70041","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.70041","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
Dear Editor,
Colorectal cancer (CRC) is a major global health issue with a 40% 5-year mortality rate,1 and 30%−50% of patients still experience recurrence after curative resection.2, 3 The clinical utility of molecular residual disease (MRD) detection in risk stratification and recurrence detection using circulating tumour DNA (ctDNA) noninvasively has attracted widespread attention but with limited studies.4-7 We measured the value of tumour-agnostic ctDNA-guided MRD for recurrence prediction and monitoring, and explored the biological characteristics of ctDNA from MRD.
We included 104 patients with stage I-IV CRC (Figure S1), aged 26 to 82 years. Fourteen (13.5%) patients had positive landmark MRD, and thirty-two (30.8%) patients had positive longitudinal MRD (Table S1). The most frequently variant genes in tumour tissue were TP53, KRAS and APC (Figure S2A), while in ctDNA were KRAS, EGFR and TP53 (Figure S2B).
Patients with negative landmark MRD had a lower recurrence percentage than positive cases (11.1% vs. 57.1%, p < .001), yielding a negative predictive value (NPV) of 88.9% (Figure 1A). The latter group had a significantly higher recurrence risk (hazard ratio [HR], 7.325; p < .001, Figure 1B). As for longitudinal MRD, the recurrence percentage was higher in positive-MRD compared to negative-MRD (43.8% vs. 5.6%, p < .001), yielding a high NPV (94.4%, Figure 1C). Positive longitudinal MRD was correlated with an elevated risk of recurrence (HR: 9.385; p < .001, Figure 1D). In multivariate analysis for disease-free survival (DFS), landmark and longitudinal MRD-positive were significantly associated with increased recurrence risks (Figure 1E). Furthermore, we explored the effect of longitudinal MRD status in patients receiving and not receiving neoadjuvant therapy (NAT). In both groups, longitudinal positive-MRD patients had higher recurrence risk than negative-MRD patients (NAT: HR, 12.509, p = .011; non-NAT: HR, 9.611, p < .001; Figure S3A and B). The recurrence risk was lower in those with negative landmark ctDNA and negative longitudinal ctDNA (Figure S4A–D). Although the NPV for ctDNA was slightly higher than that for MRD, the PPV for ctDNA was lower than that for MRD. The area under the curve (AUC) of 3-year DFS for landmark MRD was .678, longitudinal MRD was .895, and landmark and longitudinal MRD had higher AUCs than ctDNA (Figure S4E). Fourteen out of 18 cases with recurrence detected MRD at the postoperative time points (Figure 1F). And 85.7% (12/14) patients had positive MRD detection before computed tomography confirmed recurrence (median: 198.5 days, Figure 1G). For MRD-positive cases, actions such as initiating adjuvant therapies, more aggressive treatment, intensified monitoring, or early intervention before clinical relapse occurs, may be clinically undertaken, potentially leading to better disease control, improved survival rates, and enhanced quality of life.
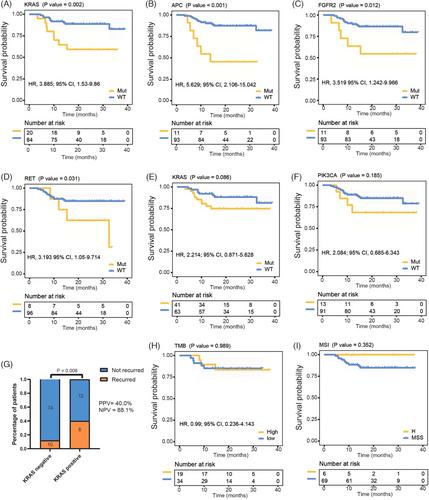
Genetic markers showed complex interactions with clinical outcomes. KRAS, APC, FGFR2 and RET variants in ctDNA were associated with inferior DFS (Figure 2A–D). In tissue, KRAS and PIK3CA variants may have the prediction potential for DFS (both p > .05, Figure 2E and F). The recurrence percentage in patients with KRAS variants in cell-free DNA (cfDNA_KRAS+) was significantly higher than those without (Figure 2G). Patients at an earlier stage exhibited a significantly better DFS (Figure S5). In the negative landmark MRD group, patients with metastases had higher variant frequencies of KRAS, ALK, RET and NTRK2 than those without (Table S2). A similar trend for these genes was observed in longitudinal MRD-negative patients (Table S3). The tumour mutation burden did not exhibit predictive capability for DFS, while the patients with high microsatellite instability tended to have a better DFS (Figure 2H and I).
The combination of MRD status with cfDNA_KRAS+ was significantly associated with patients’ outcomes. Among patients with positive landmark MRD and positive longitudinal MRD, cfDNA_KRAS+ showed a trend to poorer DFS (Figure 3A and B). In patients with negative landmark MRD, cfDNA_KRAS+ was associated with poorer DFS (Figure 3A). Then, patients with a positive result in at least one of the 2 statuses (cfDNA_KRAS variants and MRD) were designated as positive. The combination of landmark MRD and cfDNA_KRAS+, and the combination of longitudinal MRD and cfDNA_KRAS+ were significantly associated with inferior DFS (Figure 3C and D). For the 3-year DFS, the combination of landmark MRD and cfDNA_KRAS+ reached an AUC of .768, surpassing both landmark MRD (.678) and cfDNA_KRAS+ (.681). Similarly, the integration of longitudinal MRD and cfDNA_KRAS+ reached an AUC of .922, surpassing both longitudinal MRD (.895) and cfDNA_KRAS+ (.681) (Figure 3E).
The recurrence risk of MRD-positive and MRD-negative patients stratified by the adjuvant therapy (AT) was analysed. No survival benefit was observed from AT in landmark MRD-positive patients due to the limited number of patients without AT (n = 2; Figure S6A and C). Patients with AT tended to have shorter DFS and higher percentage of recurrence than patients without AT in the landmark MRD-negative group (Figure S6B and D). Adjuvant therapy may not be suitable for landmark MRD-negative CRC patients to prevent over-medicalisation.
The I/II class mutation sites and all mutation sites were predominantly concentrated in fragments below 200 bp (Figure 4A and E). Furthermore, we compared the proportion of mutation reads at different length intervals. The proportions of class I/II mutation reads and all mutation reads in the fragments ≤ 100 bp were significantly higher than those in the fragments >100 bp (Figure 4B and F). The percentages of fragments ≤ 100 bp in class I/II mutation reads and all mutation reads were higher than those in non-mutated reads (Figure 4C and G). The median length of class I/II mutation reads was lower than non-mutated reads (163 bp vs. 168 bp; Figure 4D). The median length of all mutation reads was also lower (166 bp vs. 169 bp; Figure 4H). Mutation sites were enriched in shorter fragments, which could potentially improve cfDNA detection methods, guiding the risk stratification, prognostic prediction, and monitoring of disease recurrence.
Our research underscored the remarkable prognostic value of ctDNA-based MRD monitoring in postoperative CRC patients. Notably, integrating cfDNA_KRAS variants with MRD significantly enhanced the precision of risk stratification. Furthermore, our findings revealed a trend towards enriching mutation sites within shorter cfDNA fragments, offering pivotal insights for developing advanced cfDNA detection strategies.
Jun You, Li Xiao and Linghua Yan conceived of the study plan. Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen, Haoyu Bai and Linghua Yan collected, analysed and interpreted data. Qingqi Hong, Jingtao Zhu, Hexin Lin, Yinan Chen and Haoyu Bai drafted the manuscript. Jun You, Li Xiao and Linghua Yan revised the manuscript. All authors reviewed the manuscript and had final approval of the submitted and published version.
The authors have no conflict of interest to declare.
This study was approved by the ethics committee of the corresponding hospital, and was carried out in compliance with the Declaration of Helsinki Principles. Written informed consent was obtained from all study participants.
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


