Fang-Yu Lin MD, Chan-Han Wu MD, Chi-Wei Chen MD, MS
{"title":"Bradycardia in a woman","authors":"Fang-Yu Lin MD, Chan-Han Wu MD, Chi-Wei Chen MD, MS","doi":"10.1002/emp2.13336","DOIUrl":null,"url":null,"abstract":"<p>A 75-year-old woman with a history of coronary artery disease, diabetes mellitus, and a previous stroke was found to have dyspnea and hypotension at a nursing home. She was brought to the emergency department in her baseline comatose state. Her vital signs were as follows: blood pressure 78/61 mmHg, heart rate 53 beats/min, respiratory rate 30 breaths/min, body temperature 36.7°C, and oxygen saturation of 100% while receiving oxygen via a non-rebreather mask.</p><p>An initial electrocardiogram (ECG) revealed mild ST-segment elevation in the inferior leads with reciprocal changes, suggestive of an acute ischemic event. However, the rhythm was inconclusive due to atypical T wave morphology (Figure 1). The emergency physician performed point-of-care ultrasonography (POCUS) to assess the relationship between atrial and ventricular contractions (Video 1).</p><p>POCUS identified two atrial contractions for every ventricular contraction, indicating a 2:1 second-degree atrioventricular (AV) block. ECG interpretation can be difficult when waveforms are obscured by overlapping or multifocal signals, complicating arrhythmia classification.<span><sup>1</sup></span> In cases of bradycardia, timely identification of AV blocks is crucial. When ECG findings are inconclusive, POCUS serves as an effective tool to assess AV conduction, enhancing diagnostic accuracy and guiding immediate clinical decisions.<span><sup>2</sup></span></p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13336","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13336","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
A 75-year-old woman with a history of coronary artery disease, diabetes mellitus, and a previous stroke was found to have dyspnea and hypotension at a nursing home. She was brought to the emergency department in her baseline comatose state. Her vital signs were as follows: blood pressure 78/61 mmHg, heart rate 53 beats/min, respiratory rate 30 breaths/min, body temperature 36.7°C, and oxygen saturation of 100% while receiving oxygen via a non-rebreather mask.
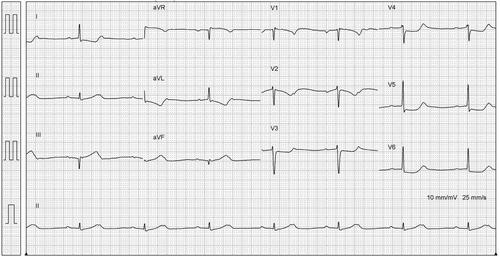
An initial electrocardiogram (ECG) revealed mild ST-segment elevation in the inferior leads with reciprocal changes, suggestive of an acute ischemic event. However, the rhythm was inconclusive due to atypical T wave morphology (Figure 1). The emergency physician performed point-of-care ultrasonography (POCUS) to assess the relationship between atrial and ventricular contractions (Video 1).
POCUS identified two atrial contractions for every ventricular contraction, indicating a 2:1 second-degree atrioventricular (AV) block. ECG interpretation can be difficult when waveforms are obscured by overlapping or multifocal signals, complicating arrhythmia classification.1 In cases of bradycardia, timely identification of AV blocks is crucial. When ECG findings are inconclusive, POCUS serves as an effective tool to assess AV conduction, enhancing diagnostic accuracy and guiding immediate clinical decisions.2

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


