{"title":"Successful transition from intravenous to inhalation anesthesia for respiratory management of coronavirus disease pneumonia: A case report","authors":"Reijiro Kato, Yuhei Irie, Yoshito Izutani, Hiroyasu Ishikura","doi":"10.1002/ams2.70010","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>In patients with coronavirus disease pneumonia, strong spontaneous breathing increases pulmonary vascular permeability and induces self-inflicted lung injury, prolonging the intensive care unit stay and worsening prognosis. Therefore, spontaneous respiration must be strictly controlled.</p>\n </section>\n \n <section>\n \n <h3> Case Presentation</h3>\n \n <p>A 48-year-old man was admitted for respiratory management of severe coronavirus disease pneumonia. Despite immediate ventilatory management, ventilatory failure and air leak syndrome developed, necessitating venovenous extracorporeal membrane oxygenation, intravenous sedation, and muscle relaxation. Over time, the patient's inspiratory effort worsened and the requirement for transvenous anesthesia increased. Therefore, management was switched to inhalation anesthesia after discontinuation of all transvenous anesthetics, maintaining morphine-only analgesia. Subsequent management enabled effective control of spontaneous respiration, allowing eventual discontinuation of inhalation anesthesia, venovenous extracorporeal membrane oxygenation, and ventilation.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Management of spontaneous respiration in coronavirus disease pneumonia can be complicated by resistance to transvenous anesthesia; however, the use of an inhaled anesthetic may present a valuable alternative.</p>\n </section>\n </div>","PeriodicalId":7196,"journal":{"name":"Acute Medicine & Surgery","volume":"11 1","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2024-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ams2.70010","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute Medicine & Surgery","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ams2.70010","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
In patients with coronavirus disease pneumonia, strong spontaneous breathing increases pulmonary vascular permeability and induces self-inflicted lung injury, prolonging the intensive care unit stay and worsening prognosis. Therefore, spontaneous respiration must be strictly controlled.
Case Presentation
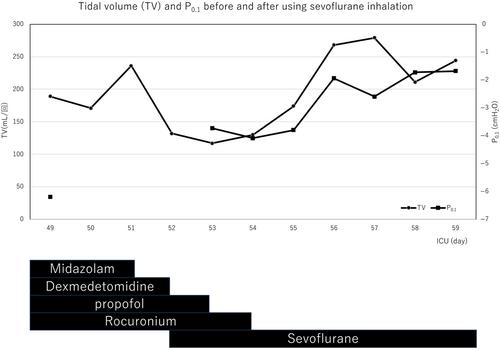
A 48-year-old man was admitted for respiratory management of severe coronavirus disease pneumonia. Despite immediate ventilatory management, ventilatory failure and air leak syndrome developed, necessitating venovenous extracorporeal membrane oxygenation, intravenous sedation, and muscle relaxation. Over time, the patient's inspiratory effort worsened and the requirement for transvenous anesthesia increased. Therefore, management was switched to inhalation anesthesia after discontinuation of all transvenous anesthetics, maintaining morphine-only analgesia. Subsequent management enabled effective control of spontaneous respiration, allowing eventual discontinuation of inhalation anesthesia, venovenous extracorporeal membrane oxygenation, and ventilation.
Conclusion
Management of spontaneous respiration in coronavirus disease pneumonia can be complicated by resistance to transvenous anesthesia; however, the use of an inhaled anesthetic may present a valuable alternative.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


