Katarina Trajkovic MD, Sanela Hasanagic MD, Dragan Vasin MD
{"title":"Man with abdominal pain following blunt trauma","authors":"Katarina Trajkovic MD, Sanela Hasanagic MD, Dragan Vasin MD","doi":"10.1002/emp2.13335","DOIUrl":null,"url":null,"abstract":"<p>A 73-year-old patient presented to the emergency department after a fall from a 3-m height, complaining of headache and light pain in the abdomen. Upon examination his vital signs were stable, his abdomen tender, and a small hematoma was observed in the left hemiabdomen. Laboratory results showed a normal bleeding profile and leukocytosis. Ultrasound examination demonstrated hyperechoic mesenteric fat. Head computed tomography (CT) showed no signs of trauma. Contrast-enhanced CT of the abdomen revealed the Janus sign (Figure 1), the complete cutoff sign (Figures 2 and 3), free fluid, and small gas particles.</p><p>The patient underwent immediate surgery: jejunal resection and sigmoid resection with terminal colostomy were performed. He recovered well and was discharged in good condition. Closing of the colostomy is planned for the end of the year.</p><p>Bowel injury is rare in blunt abdominal trauma, often presenting with few signs and symptoms.<span><sup>1</sup></span> CT is the primary imaging modality for evaluating these patients.<span><sup>2</sup></span> Bowel transection is the most severe form of bowel trauma, and the findings include the Janus sign—specific for small bowel transection, representing a hyper enhancing loop continuous with a loop that shows no or decreased enhancement, as well as the complete cutoff sign—the circular disruption of the bowel wall, specific of both small and large bowel transection.<span><sup>3</sup></span> Knowledge and prompt observance of these signs, as well as of nonspecific findings, such as pneumoperitoneum or free fluid, is the key to the correct diagnosis and timely surgical treatment.</p><p>The authors declare they have no conflicts of interest.</p>","PeriodicalId":73967,"journal":{"name":"Journal of the American College of Emergency Physicians open","volume":"5 5","pages":""},"PeriodicalIF":1.9000,"publicationDate":"2024-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/emp2.13335","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the American College of Emergency Physicians open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/emp2.13335","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
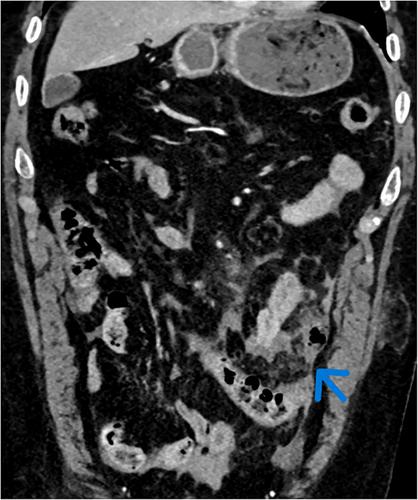
A 73-year-old patient presented to the emergency department after a fall from a 3-m height, complaining of headache and light pain in the abdomen. Upon examination his vital signs were stable, his abdomen tender, and a small hematoma was observed in the left hemiabdomen. Laboratory results showed a normal bleeding profile and leukocytosis. Ultrasound examination demonstrated hyperechoic mesenteric fat. Head computed tomography (CT) showed no signs of trauma. Contrast-enhanced CT of the abdomen revealed the Janus sign (Figure 1), the complete cutoff sign (Figures 2 and 3), free fluid, and small gas particles.
The patient underwent immediate surgery: jejunal resection and sigmoid resection with terminal colostomy were performed. He recovered well and was discharged in good condition. Closing of the colostomy is planned for the end of the year.
Bowel injury is rare in blunt abdominal trauma, often presenting with few signs and symptoms.1 CT is the primary imaging modality for evaluating these patients.2 Bowel transection is the most severe form of bowel trauma, and the findings include the Janus sign—specific for small bowel transection, representing a hyper enhancing loop continuous with a loop that shows no or decreased enhancement, as well as the complete cutoff sign—the circular disruption of the bowel wall, specific of both small and large bowel transection.3 Knowledge and prompt observance of these signs, as well as of nonspecific findings, such as pneumoperitoneum or free fluid, is the key to the correct diagnosis and timely surgical treatment.
The authors declare they have no conflicts of interest.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


