David Gallinet, Maxime Antoni, ReSurg, Julien Berhouet, Christophe Charousset, Jacques Guery
{"title":"MRI findings and clinical testing for preoperative diagnosis of long head of the biceps pathology","authors":"David Gallinet, Maxime Antoni, ReSurg, Julien Berhouet, Christophe Charousset, Jacques Guery","doi":"10.1002/jeo2.70050","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Purpose</h3>\n \n <p>Determine whether combining magnetic resonance imaging (MRI) observations and clinical tests could substantially improve sensitivity for diagnosis of long head of the biceps tendon (LHBT) pathology.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>The authors retrospectively assessed a consecutive series of 140 patients who underwent arthroscopic rotator cuff repair for isolated supraspinatus tears. The presence of LHBT pathology was assessed preoperatively on MRI using three criteria and four clinical tests specific to shoulder injuries. Binary outcomes of MRI observations and four clinical tests were combined to identify combinations resulting in the best sensitivity using intra-operative arthroscopic findings as reference.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The study cohort comprised 100 shoulders (58 men and 42 women) aged 56.6 ± 9.4 years (range, 30–76) at index surgery. A total of 29 combinations were tested to obtain the best diagnostic algorithm for LHBT pathologies. Only four combinations reached a sensitivity ≥0.75, but had a specificity <0.45. The ‘Speed or Signal’ combination achieved the highest sensitivity (Se: 0.88; 95% confidence interval [CI]: 0.73%–0.96%; Sp: 0.20; 95% CI: 0.10%–0.33%).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The most important findings of this study were that, for the diagnosis of LHBT pathology using clinical tests alone, the Speed test had the highest sensitivity (Se, 0.74), and using MRI observations alone, the signal intensity had the highest sensitivity (Se, 0.68). Combination of ‘Speed test or Signal intensity’ substantially improved the sensitivity (Se, 0.88) but yielded the lowest specificity (Sp, 0.20). The clinical relevance of these findings is that using the combination ‘Speed or Signal’ for preoperative diagnosis, 88% of pathologic LHBTs would be correctly diagnosed, while 80% of healthy LHBTs could be misdiagnosed as pathologic.</p>\n </section>\n \n <section>\n \n <h3> Level of Evidence</h3>\n \n <p>Diagnostic study, Level IV.</p>\n </section>\n </div>","PeriodicalId":36909,"journal":{"name":"Journal of Experimental Orthopaedics","volume":"11 4","pages":""},"PeriodicalIF":2.7000,"publicationDate":"2024-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jeo2.70050","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Experimental Orthopaedics","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jeo2.70050","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose
Determine whether combining magnetic resonance imaging (MRI) observations and clinical tests could substantially improve sensitivity for diagnosis of long head of the biceps tendon (LHBT) pathology.
Methods
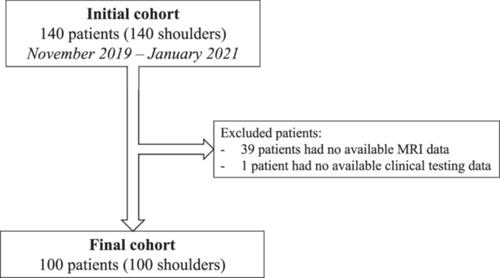
The authors retrospectively assessed a consecutive series of 140 patients who underwent arthroscopic rotator cuff repair for isolated supraspinatus tears. The presence of LHBT pathology was assessed preoperatively on MRI using three criteria and four clinical tests specific to shoulder injuries. Binary outcomes of MRI observations and four clinical tests were combined to identify combinations resulting in the best sensitivity using intra-operative arthroscopic findings as reference.
Results
The study cohort comprised 100 shoulders (58 men and 42 women) aged 56.6 ± 9.4 years (range, 30–76) at index surgery. A total of 29 combinations were tested to obtain the best diagnostic algorithm for LHBT pathologies. Only four combinations reached a sensitivity ≥0.75, but had a specificity <0.45. The ‘Speed or Signal’ combination achieved the highest sensitivity (Se: 0.88; 95% confidence interval [CI]: 0.73%–0.96%; Sp: 0.20; 95% CI: 0.10%–0.33%).
Conclusion
The most important findings of this study were that, for the diagnosis of LHBT pathology using clinical tests alone, the Speed test had the highest sensitivity (Se, 0.74), and using MRI observations alone, the signal intensity had the highest sensitivity (Se, 0.68). Combination of ‘Speed test or Signal intensity’ substantially improved the sensitivity (Se, 0.88) but yielded the lowest specificity (Sp, 0.20). The clinical relevance of these findings is that using the combination ‘Speed or Signal’ for preoperative diagnosis, 88% of pathologic LHBTs would be correctly diagnosed, while 80% of healthy LHBTs could be misdiagnosed as pathologic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


