Renal transplant nephrolithiasis: Presentation, management and follow-up with control comparisons
Abstract
Objectives
To analyse the presentation, management and long-term outcomes of renal transplant patients who formed kidney stones in their allograft. The secondary aim was to identify risk factors for stone formation in this cohort.
Materials and Methods
Patient information from an institutional renal transplant database was used to identify individuals who both did and did not form kidney stones following renal transplantation. Computerized tomography (CT) imaging was used to make the diagnosis of kidney stones and measure stone size. Age- and gender-matched controls never forming a stone in their allograft were used for comparative analysis to identify risk factors for stone formation in transplant patients.
Results
A total of 8835 transplant patients were included in the study, of which 128 (1.4%) formed a kidney stone in their allograft after surgery. The mean time to kidney stone identification was 6.2 years, and the mean number of stones formed was 1.7, with a mean maximum size dimension on a CT scan of 5.7 mm per stone. A total of 26 patients were subjected to stone-removing procedures, the most common being ureteroscopy (42.3%). The primary intervention failed in eight patients requiring a secondary intervention, and percutaneous nephrolithotomy (PCNL) had the lowest success rate (60%). A total of 164 controls were identified. In comparison to controls, stone formers had lower serum calcium (p = 0.008), lower estimated glomerular filtration rates (p = 0.019), higher lymphocyte counts (p = 0.021) and greater rate of urinary tract infection (p = 0.003). Graft failure rates were the same (p = 0.524), but time to graft failure was significantly longer in stone patients compared with controls (p = 0.008).
Conclusions
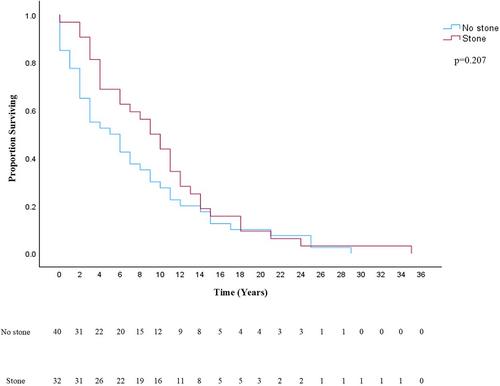
The rate of stone formation is low in transplant patients. Success rates for stone treatment vary based on the surgery selected, with PCNL being the worst. Graft survival rates were equivocal, but survival time was better in stone patients. Our analysis calls for further investigation of this important topic.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


