Gary L. Simmons, Roy Sabo, Rehan Qayyum, May Aziz, Erika Martin, Robyn J. Bernard, Manjari Sriparna, Cody McIntire, Elizabeth Krieger, Donald F. Brophy, Ramesh Natarajan, Alpha Fowler III, Catherine H. Roberts, Amir Toor
{"title":"Feasibility of intravenous vitamin C supplementation in allogeneic hematopoietic cell transplant recipients","authors":"Gary L. Simmons, Roy Sabo, Rehan Qayyum, May Aziz, Erika Martin, Robyn J. Bernard, Manjari Sriparna, Cody McIntire, Elizabeth Krieger, Donald F. Brophy, Ramesh Natarajan, Alpha Fowler III, Catherine H. Roberts, Amir Toor","doi":"10.1002/jha2.995","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Intravenous vitamin C was administered following hematopoietic stem cell transplant to mitigate nonrelapse mortality (NRM) in a Phase II clinical trial.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Patients with advanced hematologic malignancies received IV vitamin C, 50 mg/kg/day, in three divided doses on days 1–14 after HSCT, followed by 500 mg bid oral until 6 months.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>All patients enrolled (55) were deficient in vitamin C at day 0 and had restoration to normal levels. Vitamin C recipients had a trend for lower nonrelapse mortality (NRM, 11% vs. 25%, <i>p</i>-value = 0.07) compared with propensity score-matched historical controls. A similar trend toward improved survival was observed (82% vs. 62% <i>p</i> = 0.06), with no attributable grade 3 and 4 toxicities to vitamin C.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In patients undergoing allogeneic HSCT, repletion of vitamin C is feasible and may reduce NRM and improve overall survival. Randomized trials in large uniform cohorts of patients are needed to confirm the utility of this easily available and inexpensive therapy.</p>\n </section>\n </div>","PeriodicalId":72883,"journal":{"name":"EJHaem","volume":"5 5","pages":"1043-1047"},"PeriodicalIF":0.0000,"publicationDate":"2024-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jha2.995","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"EJHaem","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jha2.995","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Intravenous vitamin C was administered following hematopoietic stem cell transplant to mitigate nonrelapse mortality (NRM) in a Phase II clinical trial.
Methods
Patients with advanced hematologic malignancies received IV vitamin C, 50 mg/kg/day, in three divided doses on days 1–14 after HSCT, followed by 500 mg bid oral until 6 months.
Results
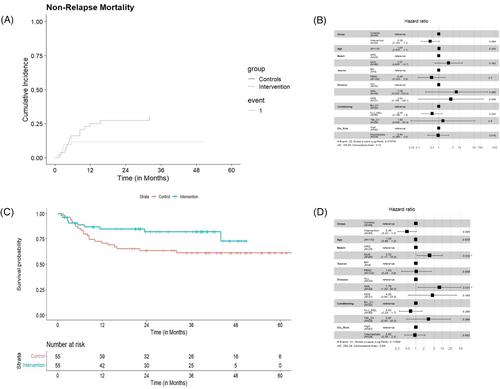
All patients enrolled (55) were deficient in vitamin C at day 0 and had restoration to normal levels. Vitamin C recipients had a trend for lower nonrelapse mortality (NRM, 11% vs. 25%, p-value = 0.07) compared with propensity score-matched historical controls. A similar trend toward improved survival was observed (82% vs. 62% p = 0.06), with no attributable grade 3 and 4 toxicities to vitamin C.
Conclusion
In patients undergoing allogeneic HSCT, repletion of vitamin C is feasible and may reduce NRM and improve overall survival. Randomized trials in large uniform cohorts of patients are needed to confirm the utility of this easily available and inexpensive therapy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


