{"title":"Vulval leiomyoma with acute postoperative delirium.","authors":"Manas Ranjan Behera, Aditya Pati, Shabnam K, Sweta Singh","doi":"10.5114/pm.2024.141094","DOIUrl":null,"url":null,"abstract":"<p><p>Leiomyomas are benign, well-circumscribed mesenchymal tumours. While uterine leiomyomas are common, vulval leiomyomas are rare. We report the challenging case of vulval leiomyoma in a multiparous woman, who also developed acute postoperative delirium. A 41-year-old multiparous woman presented with a mass in the perineum of one year duration and discomfort in a sitting position since a month ago. Her menstrual history, family history, and personal history were unremarkable. On examination of the vulva, there was a firm mass of size 10 x 8 cm on the left side, involving the labium majus and minus, which was distorting the introitus. The uterus and ovaries were normal. Preoperative ultrasound was suggestive of a vulval solid lobulated lesion, probably leiomyoma. Excision of the mass was performed. The patient developed postoperative delirium at 3 hours and was treated with an injection of haloperidol, antibiotics, and electrolyte correction. She recovered well and was discharged on the sixth postoperative day. Histopathology confirmed leiomyoma of the vulval mass, with areas of cystic degeneration. At 6-month follow-up the patient was asymptomatic and had no recurrence. To conclude, vulval leiomyoma is rare and treated by excision. The occurrence of postoperative delirium adds to the surgical morbidity, and gynaecologists should be aware of these conditions for optimal outcomes.</p>","PeriodicalId":55643,"journal":{"name":"Przeglad Menopauzalny","volume":"23 2","pages":"113-116"},"PeriodicalIF":1.7000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11462146/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Przeglad Menopauzalny","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5114/pm.2024.141094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
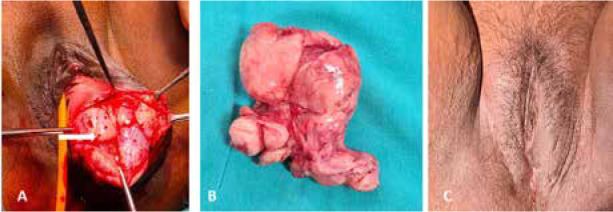
Leiomyomas are benign, well-circumscribed mesenchymal tumours. While uterine leiomyomas are common, vulval leiomyomas are rare. We report the challenging case of vulval leiomyoma in a multiparous woman, who also developed acute postoperative delirium. A 41-year-old multiparous woman presented with a mass in the perineum of one year duration and discomfort in a sitting position since a month ago. Her menstrual history, family history, and personal history were unremarkable. On examination of the vulva, there was a firm mass of size 10 x 8 cm on the left side, involving the labium majus and minus, which was distorting the introitus. The uterus and ovaries were normal. Preoperative ultrasound was suggestive of a vulval solid lobulated lesion, probably leiomyoma. Excision of the mass was performed. The patient developed postoperative delirium at 3 hours and was treated with an injection of haloperidol, antibiotics, and electrolyte correction. She recovered well and was discharged on the sixth postoperative day. Histopathology confirmed leiomyoma of the vulval mass, with areas of cystic degeneration. At 6-month follow-up the patient was asymptomatic and had no recurrence. To conclude, vulval leiomyoma is rare and treated by excision. The occurrence of postoperative delirium adds to the surgical morbidity, and gynaecologists should be aware of these conditions for optimal outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


