{"title":"Approach to Newborns with Elevated TSH: A Different Perspective from the International Guidelines for Iodine-deficient Countries","authors":"Cengiz Kara, Hüseyin Anıl Korkmaz","doi":"10.4274/jcrpe.galenos.2024.2024-4-15","DOIUrl":null,"url":null,"abstract":"<p><p>Lowering of thyroid-stimulating hormone (TSH) cutoffs in newborn screening programs has created a management dilemma by leading to more frequent detection of neonates with elevated TSH concentrations due to false-positive results, transient neonatal hyperthyrotropinemia (NHT), and milder forms of congenital hypothyroidism. Current consensus guidelines recommend starting treatment if the venous TSH level is >20 mU/L in the face of a normal free thyroxine (FT4) level, which is an arbitrary threshold for treatment decisions. In countries such as Türkiye, where transient NHT may be more common due to iodine deficiency (ID) and/or overload, putting this recommendation into daily practice may lead to unnecessary or over treatment, time-consuming long-term follow-up, and increased workload and costs. In this review, we addressed alternative approaches for infants with elevated TSH concentrations detected at newborn screening. The suggested management approach can be summarized as: Infants with mild NHT (venous TSH <20 mU/L) should be followed without treatment. In moderate NHT (venous TSH 20-30 mU/L), treatment or monitoring decisions can be made according to age, TSH trend and absolute FT4 level. Moderate cases of NHT should be treated if age at confirmatory testing is >21 days or if there is no downward trend in TSH and FT4 level is in the lower half of age-specific reference range in the first 21 days. In in-between cases of moderate NHT, thyroid ultrasound may guide treatment decision by determining mild cases of thyroid dysgenesis that require life-long treatment. Otherwise, monitoring is a reasonable option. Infants with compensated hypothyroidism (venous TSH >30 mU/L and normal FT4) or persistent hyperthyrotropinemia (>6-10 mU/L after the neonatal period) should receive L-thyroxine treatment. However, all treated cases of isolated TSH elevation should be closely monitored to avoid overtreatment, and re-evaluated by a trial off therapy. This alternative approach will largely eliminate unnecessary treatment of infants with transient NHT, mostly caused by ID or excess in Türkiye, and will reduce workload and costs by preventing unwarranted investigation and long-term follow-up.</p>","PeriodicalId":48805,"journal":{"name":"Journal of Clinical Research in Pediatric Endocrinology","volume":" ","pages":"242-255"},"PeriodicalIF":1.5000,"publicationDate":"2025-08-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372647/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Research in Pediatric Endocrinology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4274/jcrpe.galenos.2024.2024-4-15","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/8 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
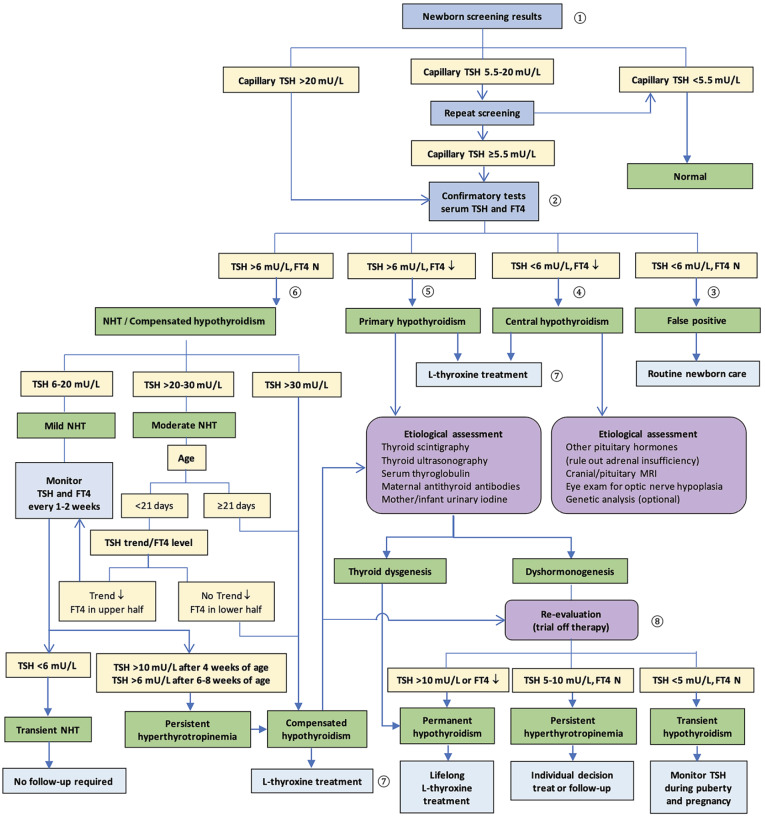
Lowering of thyroid-stimulating hormone (TSH) cutoffs in newborn screening programs has created a management dilemma by leading to more frequent detection of neonates with elevated TSH concentrations due to false-positive results, transient neonatal hyperthyrotropinemia (NHT), and milder forms of congenital hypothyroidism. Current consensus guidelines recommend starting treatment if the venous TSH level is >20 mU/L in the face of a normal free thyroxine (FT4) level, which is an arbitrary threshold for treatment decisions. In countries such as Türkiye, where transient NHT may be more common due to iodine deficiency (ID) and/or overload, putting this recommendation into daily practice may lead to unnecessary or over treatment, time-consuming long-term follow-up, and increased workload and costs. In this review, we addressed alternative approaches for infants with elevated TSH concentrations detected at newborn screening. The suggested management approach can be summarized as: Infants with mild NHT (venous TSH <20 mU/L) should be followed without treatment. In moderate NHT (venous TSH 20-30 mU/L), treatment or monitoring decisions can be made according to age, TSH trend and absolute FT4 level. Moderate cases of NHT should be treated if age at confirmatory testing is >21 days or if there is no downward trend in TSH and FT4 level is in the lower half of age-specific reference range in the first 21 days. In in-between cases of moderate NHT, thyroid ultrasound may guide treatment decision by determining mild cases of thyroid dysgenesis that require life-long treatment. Otherwise, monitoring is a reasonable option. Infants with compensated hypothyroidism (venous TSH >30 mU/L and normal FT4) or persistent hyperthyrotropinemia (>6-10 mU/L after the neonatal period) should receive L-thyroxine treatment. However, all treated cases of isolated TSH elevation should be closely monitored to avoid overtreatment, and re-evaluated by a trial off therapy. This alternative approach will largely eliminate unnecessary treatment of infants with transient NHT, mostly caused by ID or excess in Türkiye, and will reduce workload and costs by preventing unwarranted investigation and long-term follow-up.
期刊介绍:
The Journal of Clinical Research in Pediatric Endocrinology (JCRPE) publishes original research articles, reviews, short communications, letters, case reports and other special features related to the field of pediatric endocrinology. JCRPE is published in English by the Turkish Pediatric Endocrinology and Diabetes Society quarterly (March, June, September, December). The target audience is physicians, researchers and other healthcare professionals in all areas of pediatric endocrinology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


