Cost Effectiveness of Sequencing Vedolizumab as First-Line Biologic in Ulcerative Colitis and Crohn's Disease in Canada: An Analysis Using Real-World Evidence from the EVOLVE Study.
Aren Fischer, Stephen Mac, Erica Stivelman Freiman, John K Marshall, Kim Rand, Juan M Ramos-Goñi
{"title":"Cost Effectiveness of Sequencing Vedolizumab as First-Line Biologic in Ulcerative Colitis and Crohn's Disease in Canada: An Analysis Using Real-World Evidence from the EVOLVE Study.","authors":"Aren Fischer, Stephen Mac, Erica Stivelman Freiman, John K Marshall, Kim Rand, Juan M Ramos-Goñi","doi":"10.1007/s41669-024-00523-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Vedolizumab is a gut-selective anti-lymphocyte trafficking biologic indicated for the treatment of adult patients with moderately to severely active ulcerative colitis (UC) and Crohn's disease (CD) in Canada.</p><p><strong>Objective: </strong>The objective of this study was to evaluate the cost effectiveness of treatment sequencing for UC and CD from a public healthcare payer perspective, leveraging new real-world evidence from the literature and the EVOLVE study, a retrospective chart review.</p><p><strong>Methods: </strong>Using separate decision tree/Markov models to assess cost effectiveness for UC and CD, two sequencing approaches were estimated for adult patients (≥ 18 years) diagnosed with UC or CD who were biologic-naïve: vedolizumab as first-line biologic followed by anti-tumor necrosis factor (TNF)-α versus first-line anti-TNFα followed by vedolizumab. Treatment effectiveness (response and remission), surgery rates, dose escalation and regain of response and safety inputs were estimated from EVOLVE, a retrospective chart review of real-world data, and evidence synthesis from the literature, whereas costs and utilities were estimated from health technology assessment reports, clinical trials, and the literature. Biosimilar costs were used for anti-TNFα. Both models simulated a 5-year time horizon and discounted costs and outcomes at 1.5%. Probabilistic base-case analyses (n = 10,000) reported total costs (2023 Canadian dollars) and quality-adjusted life-years (QALYs). Several scenario analyses were conducted to explore robustness of results.</p><p><strong>Results: </strong>In UC, vedolizumab as a first-line biologic followed by anti-TNFα resulted in an incremental gain of 0.09 QALYs (2.46 vs. 2.55) and saved $7179 ($134,028 vs. $126,848), making this a dominant strategy compared with first-line anti-TNFα followed by vedolizumab. In CD, use of vedolizumab as a first-line biologic resulted in an incremental gain of 0.04 QALYs (3.35 vs. 3.39) at an incremental cost of $50,631 ($89,850 vs. $140,381) versus first-line anti-TNFα followed by vedolizumab (incremental cost-effectiveness ratio of $1,265,775 per QALY).</p><p><strong>Conclusions: </strong>Based on this analysis, sequencing vedolizumab as a first-line biologic prior to anti-TNFα in UC and CD provided additional clinical benefit to patients. In UC, vedolizumab as a first-line biologic also saved healthcare system costs compared with anti-TNFα, whereas in CD, vedolizumab provided incremental benefit at an incremental cost, which was not considered cost effective at a threshold of $50,000/QALY.</p>","PeriodicalId":19770,"journal":{"name":"PharmacoEconomics Open","volume":" ","pages":"41-56"},"PeriodicalIF":2.1000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11718032/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s41669-024-00523-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Vedolizumab is a gut-selective anti-lymphocyte trafficking biologic indicated for the treatment of adult patients with moderately to severely active ulcerative colitis (UC) and Crohn's disease (CD) in Canada.
Objective: The objective of this study was to evaluate the cost effectiveness of treatment sequencing for UC and CD from a public healthcare payer perspective, leveraging new real-world evidence from the literature and the EVOLVE study, a retrospective chart review.
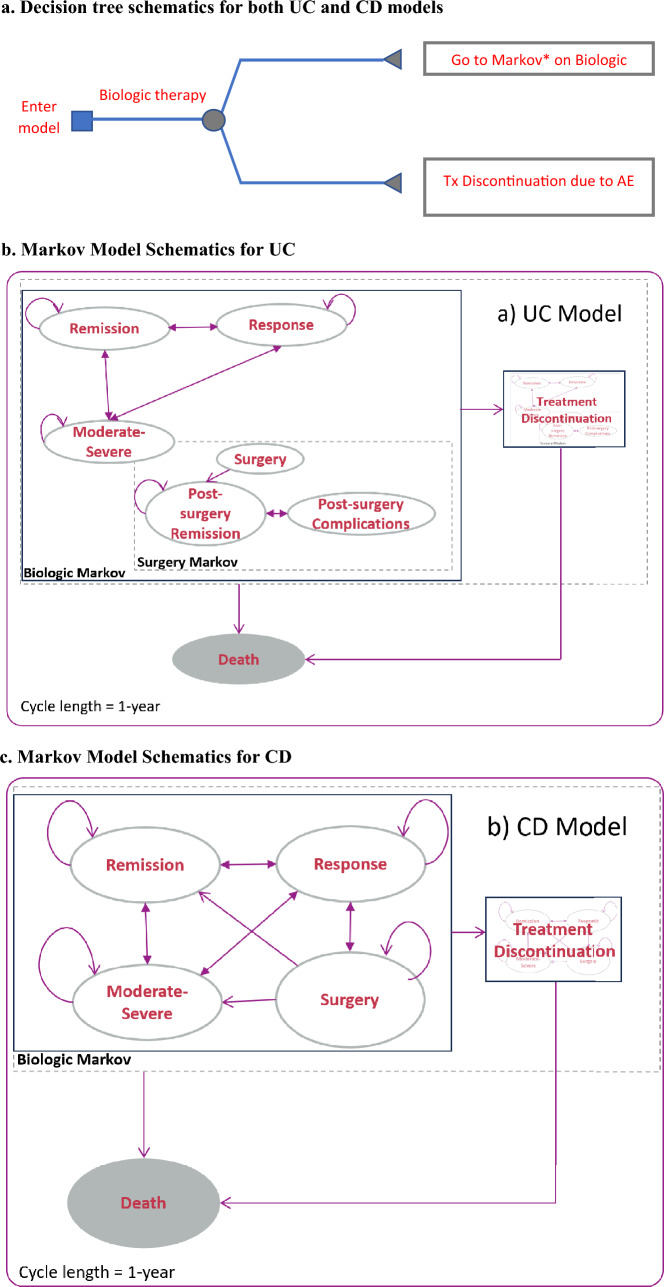
Methods: Using separate decision tree/Markov models to assess cost effectiveness for UC and CD, two sequencing approaches were estimated for adult patients (≥ 18 years) diagnosed with UC or CD who were biologic-naïve: vedolizumab as first-line biologic followed by anti-tumor necrosis factor (TNF)-α versus first-line anti-TNFα followed by vedolizumab. Treatment effectiveness (response and remission), surgery rates, dose escalation and regain of response and safety inputs were estimated from EVOLVE, a retrospective chart review of real-world data, and evidence synthesis from the literature, whereas costs and utilities were estimated from health technology assessment reports, clinical trials, and the literature. Biosimilar costs were used for anti-TNFα. Both models simulated a 5-year time horizon and discounted costs and outcomes at 1.5%. Probabilistic base-case analyses (n = 10,000) reported total costs (2023 Canadian dollars) and quality-adjusted life-years (QALYs). Several scenario analyses were conducted to explore robustness of results.
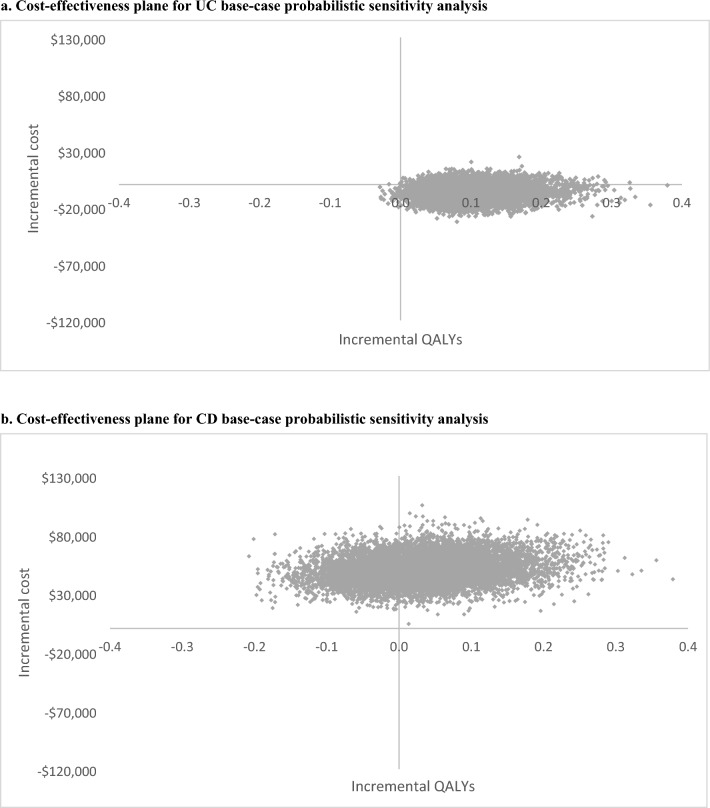
Results: In UC, vedolizumab as a first-line biologic followed by anti-TNFα resulted in an incremental gain of 0.09 QALYs (2.46 vs. 2.55) and saved $7179 ($134,028 vs. $126,848), making this a dominant strategy compared with first-line anti-TNFα followed by vedolizumab. In CD, use of vedolizumab as a first-line biologic resulted in an incremental gain of 0.04 QALYs (3.35 vs. 3.39) at an incremental cost of $50,631 ($89,850 vs. $140,381) versus first-line anti-TNFα followed by vedolizumab (incremental cost-effectiveness ratio of $1,265,775 per QALY).
Conclusions: Based on this analysis, sequencing vedolizumab as a first-line biologic prior to anti-TNFα in UC and CD provided additional clinical benefit to patients. In UC, vedolizumab as a first-line biologic also saved healthcare system costs compared with anti-TNFα, whereas in CD, vedolizumab provided incremental benefit at an incremental cost, which was not considered cost effective at a threshold of $50,000/QALY.
期刊介绍:
PharmacoEconomics - Open focuses on applied research on the economic implications and health outcomes associated with drugs, devices and other healthcare interventions. The journal includes, but is not limited to, the following research areas:Economic analysis of healthcare interventionsHealth outcomes researchCost-of-illness studiesQuality-of-life studiesAdditional digital features (including animated abstracts, video abstracts, slide decks, audio slides, instructional videos, infographics, podcasts and animations) can be published with articles; these are designed to increase the visibility, readership and educational value of the journal’s content. In addition, articles published in PharmacoEconomics -Open may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand important medical advances.All manuscripts are subject to peer review by international experts. Letters to the Editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


