Aditya Sakalkale MBBCh, BAO, Shriranshini Satheakeerthy MBBS, MTrauma, Justin M. C. Yeung FRCSEd (Gen Surg), FRACS, Fiona Reid BMBS, FRACS
{"title":"From research to teaching: enhancing prevocational surgical training with part-time contracts","authors":"Aditya Sakalkale MBBCh, BAO, Shriranshini Satheakeerthy MBBS, MTrauma, Justin M. C. Yeung FRCSEd (Gen Surg), FRACS, Fiona Reid BMBS, FRACS","doi":"10.1111/ans.19267","DOIUrl":null,"url":null,"abstract":"<p>Surgical training remains a challenging career pathway. Prevocational registrars fill service roles and spend time outside clinical duties, building upon their Surgical Education and Training (SET) applications, the accredited surgical training programme in Australasia. Balancing clinical responsibilities with academic endeavours demands meticulous organization. Research projects, didactic teaching and higher education such as a Masters or PhD, are difficult to complete whilst working full-time. Over the years, prevocational surgical registrars increasingly leave full-time employment (FTE) to achieve their desired portfolio. Leaving FTE could mean difficulty in sustaining mentorship, lack of academic structure, loss of clinical and technical skills, as well as financial constraints.<span><sup>1-3</sup></span> To the hospital, the loss of a surgical registrar from FTE to a non-clinical research year creates rostering issues and disruptions to surgical units. With the Royal Australasian College of Surgeons (RACS) supporting flexible hours among SET as well as prevocational trainees (usually post-graduate years 3–6+), hybrid employment may be necessary to address workforce needs and help trainees achieve their goals.<span><sup>2, 4</sup></span></p><p>Flexible training has been implemented for over a decade in SET trainees,<span><sup>5</sup></span> with 26 out of 1264 adopting part-time training in 2022.<span><sup>6</sup></span> However, literature is porous regarding the ‘lost tribe’ of prevocational doctors. Utilizing the <i>‘Flexible Training Toolkit’</i> published by RACS,<span><sup>7</sup></span> our institution created two standalone 0.5 full-time employment positions to address prevocational registrar attrition. The purpose of these positions is to guide trainees in meeting the selection criteria for SET and to maintain fundamental clinical skills. Part-academic prevocational roles have been implemented in PGY1 and 2 years in the United Kingdom and the Republic of Ireland with some success.<span><sup>8-10</sup></span> The hope is to emulate this success in senior positions. Whilst not a guarantee of SET training acceptance, it certainly focuses the trainee towards obtaining required research publications, presentations and at least 12 months of dedicated medical student teaching requirements.</p><p>The roles are set up as a 12-month contract, allowing for alternating three-month clinical / three-month non-clinical terms aligned with hospital-wide term rotation, or a six-month clinical / six-month non-clinical arrangement. A clinical term includes either working day shifts in a designated general surgical unit for a full term and performing all duties as normal for the unit to function (scrubbing for cases, admitting new patients and taking consults), or a reliever term, covering SET trainee leave, covering night duty and gaps in rostering. Bolstering the workforce pool with additional registrars familiar with the system rather than recruiting externally. The non-clinical terms are free-from and organized as the registrar sees fit to meet pre-determined milestones (discussed with the consultant supervisors of this role). An example of a non-clinical week is presented in Figure 1. These milestones are re-evaluated every few weeks by supervisor-trainee meetings. Weekly composition varies between completing research project tasks like ethics proposals for randomized control trials and teaching responsibilities for junior doctors or medical students. Non-clinical terms are not institutionally funded. Trainees must sustain themselves without regular income or take on locum shifts. Arrangements were made to suit their financial needs, that is, 3 months of non-clinical requiring fewer locum shifts compared to 6 months. Medical administration was consulted, and contracts were drawn to preserve long-service entitlements. While gaps in local workforce rosters have made this model sustainable, there is hope that non-clinical roles will generate a small wage in future. The specific agreement secured a university-backed research stipend and an institutional stipend to ease some of the financial strain, covering research-related expenses such as conference fees, journal fees, statistician fees and hardware such as laptops.</p><p>Whilst there are financial drawbacks to the trainee, there are multiple advantages to part-time roles (known as ‘Less than full-time’ [LTFT] internationally) as shown in qualitative research.<span><sup>3, 11</sup></span> Trainees can more effectively conduct higher-quality research such as randomized control trials, systematic reviews or retrospective studies in a timely fashion. Prevocational trainees are also empowered to use this part-time arrangement for personal progress such as family planning.<span><sup>2, 3</sup></span> Opportunities arise for involvement in long-term projects such as prospective studies and clinical trials by being involved with the larger academic community. Collaboration with researchers becomes far more feasible when not on clinical duties. There is also a provision to pursue postgraduate research degrees. For junior researchers entering academia, the starting point for research can be unclear. To assist, an academic unit with university-affiliated statisticians, data scientists, REDCap analysts, and research clinicians is available for consultation, all of whom contribute to the success of publications.</p><p>Establishing this supernumerary role required years of planning. Ultimately requiring trust and shared vision among the medical executive, university-linked professor of surgery, and the training director. The first step included recognizing recruitment issues, acknowledging the conflicting issues of strained service provisions now, and the value of investing time and effort early in the future workforce. During recruitment interviews, assessments were conducted on the perspectives regarding flexible training and the interest in flexible working arrangements. The findings indicated a significant interest in part-time work opportunities, demonstrating the necessity for the establishment of this role. A business case was put forward towards Hospital leadership stating the potential benefits of flexible options included high-level research output (linked with superior mortality rates on a hospital level), investing in surgical education for junior doctors and international data that positively correlates realized human capital and training investment to the retention of employees.<span><sup>12, 13</sup></span> There was also scope to leverage re-allocated unit overtime to help fund this position.<span><sup>7</sup></span> Acknowledging the potential supervisory issues and to foster a supported working environment with part-time staff the decision was made to recruit from the internal pool only and place the clinical job within the colorectal unit to which both the DCT and Professor of Surgery belong. The role's success is largely attributable to this intensive level of oversight. This presentation led to senior leadership support, a financial stipend, and capital resources. Feedback about this arrangement has been positive, from the SET trainees, the medical workforce unit, the multiple surgical units and the trainees in the roles themselves.</p><p>RACS upholds a progressive stance on flexible training, recognizing its pivotal role in nurturing well-rounded and adaptable surgical trainees.<span><sup>7</sup></span> Embracing the evolving landscape of medical education and workforce demands, RACS advocates for flexible training pathways that accommodate diverse career trajectories and personal circumstances. As of 2018, 75% of hospitals supported flexible training for SET trainees (only 2% of SET trainees occupy part-time roles), we have expanded the ‘<i>Flexible Training Toolkit</i>’ to include prevocational registrars.<span><sup>6, 7, 14</sup></span> Through tailored programs and supportive frameworks, RACS endeavours to foster a culture of inclusivity, innovation, and continuous professional development among its trainees, empowering them to thrive in an ever-changing healthcare environment.<span><sup>14</sup></span> and uphold clinical proficiency.</p><p>With the increasing demands and requirements for entering SET training, it is important to expand structured, flexible roles to prevocational registrars to support building a strong CV. Perhaps this opens the forum to discuss whether these measures taken by institutions are truly necessary to produce effective clinicians. Many would agree that sensitivity to recency of practice, duration and quality of training are critical to a successful surgical career. Non-clinical time for high-quality research and teaching within a structured framework, while maintaining ongoing clinical exposure, alongside highly supported training jobs in ‘clinical time’ is a worthwhile effort. Hopefully, the approach described may inspire the creation of similar opportunities for junior surgical registrars in other health networks.</p><p><b>Aditya Sakalkale:</b> Formal analysis; investigation; writing – original draft; writing – review and editing. <b>Shriranshini Satheakeerthy:</b> Methodology; writing – review and editing. <b>Justin M. C. Yeung:</b> Conceptualization; supervision; writing – review and editing. <b>Fiona Reid:</b> Conceptualization; supervision; writing – review and editing.</p>","PeriodicalId":8158,"journal":{"name":"ANZ Journal of Surgery","volume":"94 11","pages":"1891-1893"},"PeriodicalIF":1.5000,"publicationDate":"2024-10-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/ans.19267","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ANZ Journal of Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/ans.19267","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Surgical training remains a challenging career pathway. Prevocational registrars fill service roles and spend time outside clinical duties, building upon their Surgical Education and Training (SET) applications, the accredited surgical training programme in Australasia. Balancing clinical responsibilities with academic endeavours demands meticulous organization. Research projects, didactic teaching and higher education such as a Masters or PhD, are difficult to complete whilst working full-time. Over the years, prevocational surgical registrars increasingly leave full-time employment (FTE) to achieve their desired portfolio. Leaving FTE could mean difficulty in sustaining mentorship, lack of academic structure, loss of clinical and technical skills, as well as financial constraints.1-3 To the hospital, the loss of a surgical registrar from FTE to a non-clinical research year creates rostering issues and disruptions to surgical units. With the Royal Australasian College of Surgeons (RACS) supporting flexible hours among SET as well as prevocational trainees (usually post-graduate years 3–6+), hybrid employment may be necessary to address workforce needs and help trainees achieve their goals.2, 4
Flexible training has been implemented for over a decade in SET trainees,5 with 26 out of 1264 adopting part-time training in 2022.6 However, literature is porous regarding the ‘lost tribe’ of prevocational doctors. Utilizing the ‘Flexible Training Toolkit’ published by RACS,7 our institution created two standalone 0.5 full-time employment positions to address prevocational registrar attrition. The purpose of these positions is to guide trainees in meeting the selection criteria for SET and to maintain fundamental clinical skills. Part-academic prevocational roles have been implemented in PGY1 and 2 years in the United Kingdom and the Republic of Ireland with some success.8-10 The hope is to emulate this success in senior positions. Whilst not a guarantee of SET training acceptance, it certainly focuses the trainee towards obtaining required research publications, presentations and at least 12 months of dedicated medical student teaching requirements.
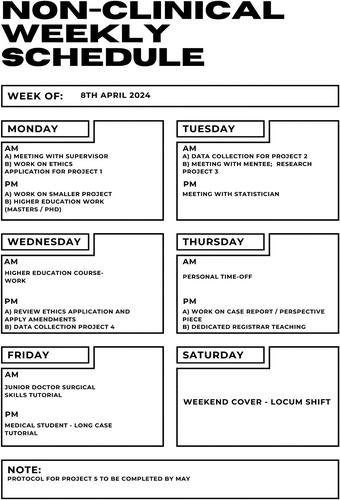
The roles are set up as a 12-month contract, allowing for alternating three-month clinical / three-month non-clinical terms aligned with hospital-wide term rotation, or a six-month clinical / six-month non-clinical arrangement. A clinical term includes either working day shifts in a designated general surgical unit for a full term and performing all duties as normal for the unit to function (scrubbing for cases, admitting new patients and taking consults), or a reliever term, covering SET trainee leave, covering night duty and gaps in rostering. Bolstering the workforce pool with additional registrars familiar with the system rather than recruiting externally. The non-clinical terms are free-from and organized as the registrar sees fit to meet pre-determined milestones (discussed with the consultant supervisors of this role). An example of a non-clinical week is presented in Figure 1. These milestones are re-evaluated every few weeks by supervisor-trainee meetings. Weekly composition varies between completing research project tasks like ethics proposals for randomized control trials and teaching responsibilities for junior doctors or medical students. Non-clinical terms are not institutionally funded. Trainees must sustain themselves without regular income or take on locum shifts. Arrangements were made to suit their financial needs, that is, 3 months of non-clinical requiring fewer locum shifts compared to 6 months. Medical administration was consulted, and contracts were drawn to preserve long-service entitlements. While gaps in local workforce rosters have made this model sustainable, there is hope that non-clinical roles will generate a small wage in future. The specific agreement secured a university-backed research stipend and an institutional stipend to ease some of the financial strain, covering research-related expenses such as conference fees, journal fees, statistician fees and hardware such as laptops.
Whilst there are financial drawbacks to the trainee, there are multiple advantages to part-time roles (known as ‘Less than full-time’ [LTFT] internationally) as shown in qualitative research.3, 11 Trainees can more effectively conduct higher-quality research such as randomized control trials, systematic reviews or retrospective studies in a timely fashion. Prevocational trainees are also empowered to use this part-time arrangement for personal progress such as family planning.2, 3 Opportunities arise for involvement in long-term projects such as prospective studies and clinical trials by being involved with the larger academic community. Collaboration with researchers becomes far more feasible when not on clinical duties. There is also a provision to pursue postgraduate research degrees. For junior researchers entering academia, the starting point for research can be unclear. To assist, an academic unit with university-affiliated statisticians, data scientists, REDCap analysts, and research clinicians is available for consultation, all of whom contribute to the success of publications.
Establishing this supernumerary role required years of planning. Ultimately requiring trust and shared vision among the medical executive, university-linked professor of surgery, and the training director. The first step included recognizing recruitment issues, acknowledging the conflicting issues of strained service provisions now, and the value of investing time and effort early in the future workforce. During recruitment interviews, assessments were conducted on the perspectives regarding flexible training and the interest in flexible working arrangements. The findings indicated a significant interest in part-time work opportunities, demonstrating the necessity for the establishment of this role. A business case was put forward towards Hospital leadership stating the potential benefits of flexible options included high-level research output (linked with superior mortality rates on a hospital level), investing in surgical education for junior doctors and international data that positively correlates realized human capital and training investment to the retention of employees.12, 13 There was also scope to leverage re-allocated unit overtime to help fund this position.7 Acknowledging the potential supervisory issues and to foster a supported working environment with part-time staff the decision was made to recruit from the internal pool only and place the clinical job within the colorectal unit to which both the DCT and Professor of Surgery belong. The role's success is largely attributable to this intensive level of oversight. This presentation led to senior leadership support, a financial stipend, and capital resources. Feedback about this arrangement has been positive, from the SET trainees, the medical workforce unit, the multiple surgical units and the trainees in the roles themselves.
RACS upholds a progressive stance on flexible training, recognizing its pivotal role in nurturing well-rounded and adaptable surgical trainees.7 Embracing the evolving landscape of medical education and workforce demands, RACS advocates for flexible training pathways that accommodate diverse career trajectories and personal circumstances. As of 2018, 75% of hospitals supported flexible training for SET trainees (only 2% of SET trainees occupy part-time roles), we have expanded the ‘Flexible Training Toolkit’ to include prevocational registrars.6, 7, 14 Through tailored programs and supportive frameworks, RACS endeavours to foster a culture of inclusivity, innovation, and continuous professional development among its trainees, empowering them to thrive in an ever-changing healthcare environment.14 and uphold clinical proficiency.
With the increasing demands and requirements for entering SET training, it is important to expand structured, flexible roles to prevocational registrars to support building a strong CV. Perhaps this opens the forum to discuss whether these measures taken by institutions are truly necessary to produce effective clinicians. Many would agree that sensitivity to recency of practice, duration and quality of training are critical to a successful surgical career. Non-clinical time for high-quality research and teaching within a structured framework, while maintaining ongoing clinical exposure, alongside highly supported training jobs in ‘clinical time’ is a worthwhile effort. Hopefully, the approach described may inspire the creation of similar opportunities for junior surgical registrars in other health networks.
Aditya Sakalkale: Formal analysis; investigation; writing – original draft; writing – review and editing. Shriranshini Satheakeerthy: Methodology; writing – review and editing. Justin M. C. Yeung: Conceptualization; supervision; writing – review and editing. Fiona Reid: Conceptualization; supervision; writing – review and editing.
期刊介绍:
ANZ Journal of Surgery is published by Wiley on behalf of the Royal Australasian College of Surgeons to provide a medium for the publication of peer-reviewed original contributions related to clinical practice and/or research in all fields of surgery and related disciplines. It also provides a programme of continuing education for surgeons. All articles are peer-reviewed by at least two researchers expert in the field of the submitted paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


