Aidan M Kirkham, Jasmine Candeliere, Sudhir K Nagpal, Henry T Stelfox, Dalibor Kubelik, George Hajjar, Derek R MacFadden, Daniel I McIsaac, Derek J Roberts
{"title":"A systematic review and meta-analysis of outcomes associated with development of surgical site infection after lower-limb revascularization surgery.","authors":"Aidan M Kirkham, Jasmine Candeliere, Sudhir K Nagpal, Henry T Stelfox, Dalibor Kubelik, George Hajjar, Derek R MacFadden, Daniel I McIsaac, Derek J Roberts","doi":"10.1177/17085381241290039","DOIUrl":null,"url":null,"abstract":"<p><p>ObjectivesAlthough surgical site infection (SSI) is a commonly used quality metric after lower-limb revascularization surgery, outcomes associated with development of this complication are poorly characterized. We conducted a systematic review and meta-analysis of studies reporting associations between development of an SSI after these procedures and clinical outcomes and healthcare resource use.MethodsWe searched MEDLINE, Embase, CENTRAL, and Evidence-Based Medicine Reviews (inception to April 4th, 2023) for studies examining adjusted associations between development of an SSI after lower-limb revascularization surgery and clinical outcomes and healthcare resource use. Two investigators independently screened abstracts and full-text citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Heterogeneity was assessed using I<sup>2</sup> statistics. GRADE was used to assess estimate certainty.ResultsAmong 6671 citations identified, we included 11 studies (n = 61,628 total patients) that reported adjusted-associations between development of an SSI and 13 different outcomes. Developing an SSI was associated with an increased adjusted-risk of hospital readmission (pooled adjusted-risk ratio (aRR) = 3.55; 95% CI (confidence interval) = 1.40-8.97; n = 4 studies; n = 13,532 patients; I<sup>2</sup> = 99.0%; moderate certainty), bypass graft thrombosis within 30-days (pooled aRR = 2.09; 95% CI = 1.41-3.09; n = 2 studies; n = 23,240 patients; I<sup>2</sup> = 51.1%; low certainty), reoperation (pooled aRR = 2.69; 95% CI = 2.67-2.72; n = 2 studies; n = 23,240 patients; I<sup>2</sup> = 0.0%; moderate certainty), bleeding requiring a transfusion or secondary procedure (aRR = 1.40; 95% CI = 1.26-1.55; n = 1 study; n = 10,910 patients; low certainty), myocardial infarction or stroke (aRR = 1.21; 95% CI = 1.02-1.43; n = 1 study; n = 10,910 patients; low certainty), and major (i.e., above-ankle) amputation (pooled aRR = 1.93; 95% CI = 1.26-2.95; n = 4 studies; n = 32,859 patients; I<sup>2</sup> = 83.0; low certainty). Development of an SSI >30-days after the index operation (aRR = 2.20; 95% CI = 1.16-4.17; n = 3 studies; n = 21,949 patients; low certainty) and prosthetic graft infection (aRR = 6.72; 95% CI = 3.21-12.70; n = 1 study; n = 272 patients; low certainty) were both associated with an increased adjusted-risk of major amputation. Prosthetic graft infection was also associated with an increased adjusted-risk of mortality >30-days after the index procedure (aRR = 6.40; 95% CI = 3.32-12.36; n = 1 study; n = 272 patients; low certainty).ConclusionsThis systematic review and meta-analysis suggests that development of an SSI after lower-limb revascularization surgery significantly increases patient morbidity and healthcare resource use. SSI is therefore a valuable quality metric after these surgeries. However, current estimates are based on heterogenous, low-to-moderate certainty evidence and should be confirmed by large, multicenter, cohort studies.</p>","PeriodicalId":23549,"journal":{"name":"Vascular","volume":" ","pages":"1150-1161"},"PeriodicalIF":0.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450249/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Vascular","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17085381241290039","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/3 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
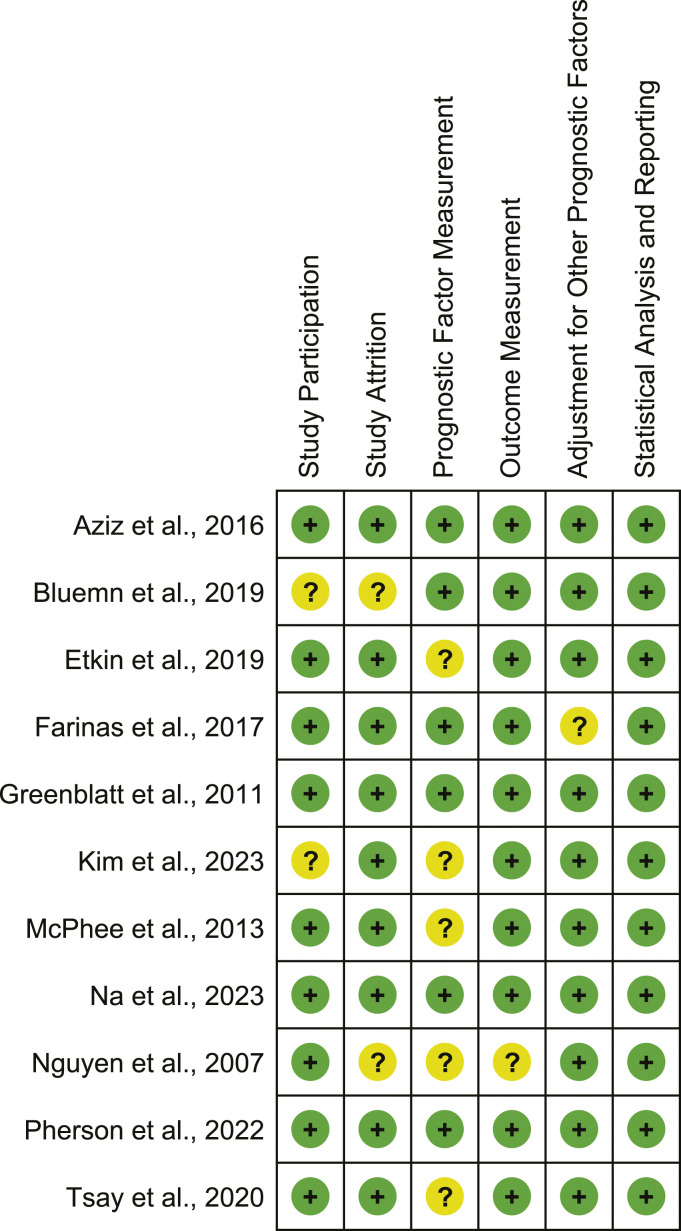
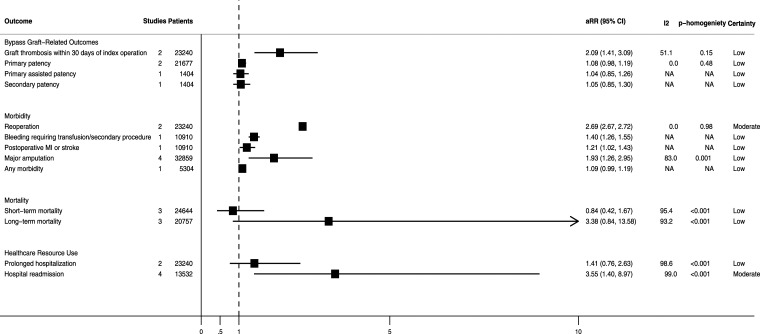
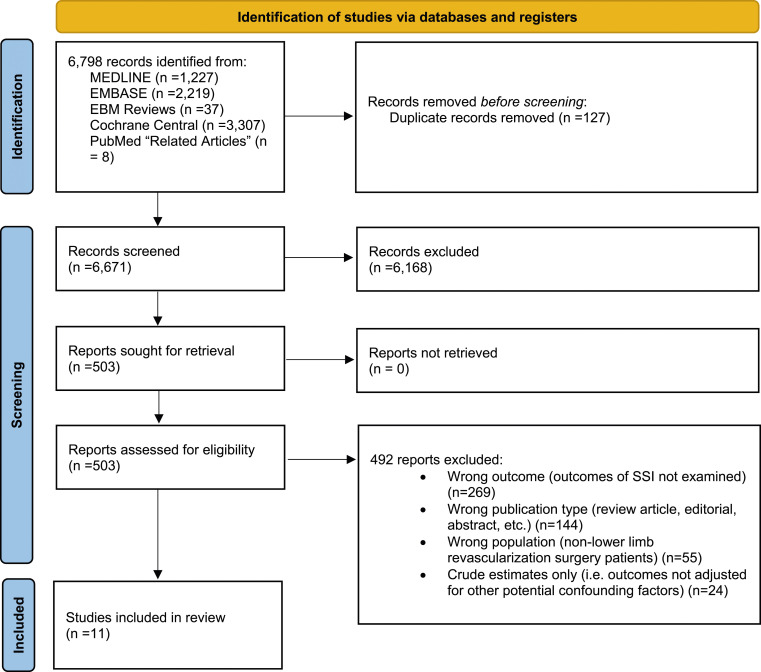
ObjectivesAlthough surgical site infection (SSI) is a commonly used quality metric after lower-limb revascularization surgery, outcomes associated with development of this complication are poorly characterized. We conducted a systematic review and meta-analysis of studies reporting associations between development of an SSI after these procedures and clinical outcomes and healthcare resource use.MethodsWe searched MEDLINE, Embase, CENTRAL, and Evidence-Based Medicine Reviews (inception to April 4th, 2023) for studies examining adjusted associations between development of an SSI after lower-limb revascularization surgery and clinical outcomes and healthcare resource use. Two investigators independently screened abstracts and full-text citations, extracted data, and assessed risk of bias. Data were pooled using random-effects models. Heterogeneity was assessed using I2 statistics. GRADE was used to assess estimate certainty.ResultsAmong 6671 citations identified, we included 11 studies (n = 61,628 total patients) that reported adjusted-associations between development of an SSI and 13 different outcomes. Developing an SSI was associated with an increased adjusted-risk of hospital readmission (pooled adjusted-risk ratio (aRR) = 3.55; 95% CI (confidence interval) = 1.40-8.97; n = 4 studies; n = 13,532 patients; I2 = 99.0%; moderate certainty), bypass graft thrombosis within 30-days (pooled aRR = 2.09; 95% CI = 1.41-3.09; n = 2 studies; n = 23,240 patients; I2 = 51.1%; low certainty), reoperation (pooled aRR = 2.69; 95% CI = 2.67-2.72; n = 2 studies; n = 23,240 patients; I2 = 0.0%; moderate certainty), bleeding requiring a transfusion or secondary procedure (aRR = 1.40; 95% CI = 1.26-1.55; n = 1 study; n = 10,910 patients; low certainty), myocardial infarction or stroke (aRR = 1.21; 95% CI = 1.02-1.43; n = 1 study; n = 10,910 patients; low certainty), and major (i.e., above-ankle) amputation (pooled aRR = 1.93; 95% CI = 1.26-2.95; n = 4 studies; n = 32,859 patients; I2 = 83.0; low certainty). Development of an SSI >30-days after the index operation (aRR = 2.20; 95% CI = 1.16-4.17; n = 3 studies; n = 21,949 patients; low certainty) and prosthetic graft infection (aRR = 6.72; 95% CI = 3.21-12.70; n = 1 study; n = 272 patients; low certainty) were both associated with an increased adjusted-risk of major amputation. Prosthetic graft infection was also associated with an increased adjusted-risk of mortality >30-days after the index procedure (aRR = 6.40; 95% CI = 3.32-12.36; n = 1 study; n = 272 patients; low certainty).ConclusionsThis systematic review and meta-analysis suggests that development of an SSI after lower-limb revascularization surgery significantly increases patient morbidity and healthcare resource use. SSI is therefore a valuable quality metric after these surgeries. However, current estimates are based on heterogenous, low-to-moderate certainty evidence and should be confirmed by large, multicenter, cohort studies.
期刊介绍:
Vascular provides readers with new and unusual up-to-date articles and case reports focusing on vascular and endovascular topics. It is a highly international forum for the discussion and debate of all aspects of this distinct surgical specialty. It also features opinion pieces, literature reviews and controversial issues presented from various points of view.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


