Bilateral Ultrasound-Guided Erector Spinae Plane Block for Management of Acute Postoperative Surgical Pain After Pediatric Cardiac Surgeries Through a Midline Sternotomy.
Mona M Mogahed, Mohamed S Abd El-Ghaffar, Mohamed S Elkahwagy
{"title":"Bilateral Ultrasound-Guided Erector Spinae Plane Block for Management of Acute Postoperative Surgical Pain After Pediatric Cardiac Surgeries Through a Midline Sternotomy.","authors":"Mona M Mogahed, Mohamed S Abd El-Ghaffar, Mohamed S Elkahwagy","doi":"10.4103/aca.aca_210_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ultrasound (US) guided erector spinae plane block (ESPB) is a safe and effective technique in providing perioperative pain management in pediatrics with a high success rate.</p><p><strong>The aim of this study: </strong>Was to compare the efficacy of bilateral ultrasound-guided erector spinae plane block for management of acute postoperative surgical pain after pediatric cardiac surgeries through a midline sternotomy.</p><p><strong>Methods: </strong>One hundred patients aged 4-12 years were randomly assigned into two groups, both groups received general anesthesia followed by bilateral sham erector spinae plane block at the level of T6 transverse process using 0.4 ml/kg normal saline on each side in the control group (group C) or bilateral ultrasound-guided erector spinae plane block at the level of T6 transverse process using 0.4 ml/kg ropivacaine 0.2% with a maximum dose of 2 mg/kg mixed with adrenaline 2 mcg/ml in erector spinae plane block group (group E). The postoperative pain scores were evaluated immediately post-extubation, at 1 hour, 2, 4, 6, 8, 10, 12, 14, 16, 18, 20, 22, and 24 hours after extubation, total consumption of intraoperative fentanyl and time to first rescue analgesic administration were also recorded.</p><p><strong>Results: </strong>There was a statistically high significant delay in the group E (314.72 ± 45.94) compared with the group C (36.7 ± 7.22) as regards to the mean (SD) of the time of the rescue analgesia (P < 0.001) (with 95% CI), moreover; the number of rescue analgesic was significantly higher in the group C compared with the group E (P < 0.001) (with 95% CI) and the mean (SD) of total intraoperative and postoperative levels fentanyl requirements in the group C were significantly higher compared with the group E (6.47 ± 0.98 and 5.09 ± 0.83) (with 95% CI) in group C versus (4.69 ± 0.71 and 2.31 ± 0.66) (with 95% CI) in group E respectively (P < 0.001) (with 95% CI).</p><p><strong>Conclusion: </strong>Ultrasound-guided bilateral ESPB with ropivacaine and adrenaline delays the postoperative need of analgesia and reduces postoperative fentanyl consumption at 24 h in pediatric patients undergoing cardiac surgery through midline sternotomy.</p>","PeriodicalId":7997,"journal":{"name":"Annals of Cardiac Anaesthesia","volume":"27 4","pages":"316-323"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11610791/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Cardiac Anaesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aca.aca_210_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/4 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Ultrasound (US) guided erector spinae plane block (ESPB) is a safe and effective technique in providing perioperative pain management in pediatrics with a high success rate.
The aim of this study: Was to compare the efficacy of bilateral ultrasound-guided erector spinae plane block for management of acute postoperative surgical pain after pediatric cardiac surgeries through a midline sternotomy.
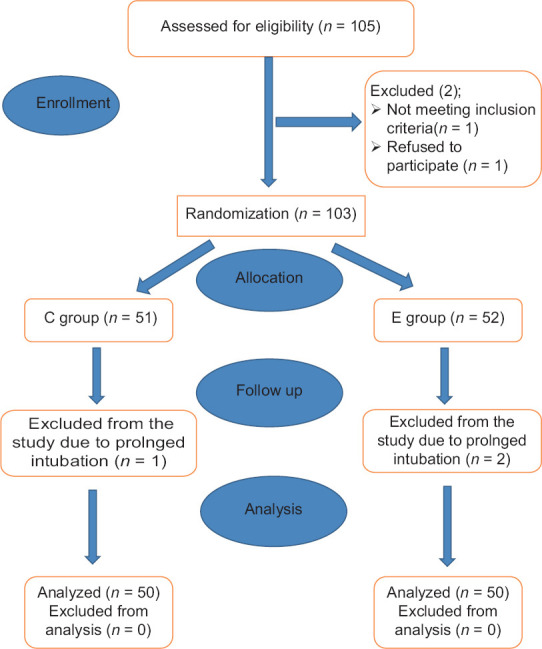
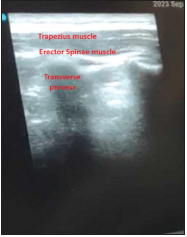
Methods: One hundred patients aged 4-12 years were randomly assigned into two groups, both groups received general anesthesia followed by bilateral sham erector spinae plane block at the level of T6 transverse process using 0.4 ml/kg normal saline on each side in the control group (group C) or bilateral ultrasound-guided erector spinae plane block at the level of T6 transverse process using 0.4 ml/kg ropivacaine 0.2% with a maximum dose of 2 mg/kg mixed with adrenaline 2 mcg/ml in erector spinae plane block group (group E). The postoperative pain scores were evaluated immediately post-extubation, at 1 hour, 2, 4, 6, 8, 10, 12, 14, 16, 18, 20, 22, and 24 hours after extubation, total consumption of intraoperative fentanyl and time to first rescue analgesic administration were also recorded.
Results: There was a statistically high significant delay in the group E (314.72 ± 45.94) compared with the group C (36.7 ± 7.22) as regards to the mean (SD) of the time of the rescue analgesia (P < 0.001) (with 95% CI), moreover; the number of rescue analgesic was significantly higher in the group C compared with the group E (P < 0.001) (with 95% CI) and the mean (SD) of total intraoperative and postoperative levels fentanyl requirements in the group C were significantly higher compared with the group E (6.47 ± 0.98 and 5.09 ± 0.83) (with 95% CI) in group C versus (4.69 ± 0.71 and 2.31 ± 0.66) (with 95% CI) in group E respectively (P < 0.001) (with 95% CI).
Conclusion: Ultrasound-guided bilateral ESPB with ropivacaine and adrenaline delays the postoperative need of analgesia and reduces postoperative fentanyl consumption at 24 h in pediatric patients undergoing cardiac surgery through midline sternotomy.
期刊介绍:
Annals of Cardiac Anaesthesia (ACA) is the official journal of the Indian Association of Cardiovascular Thoracic Anaesthesiologists. The journal is indexed with PubMed/MEDLINE, Excerpta Medica/EMBASE, IndMed and MedInd. The journal’s full text is online at www.annals.in. With the aim of faster and better dissemination of knowledge, we will be publishing articles ‘Ahead of Print’ immediately on acceptance. In addition, the journal would allow free access (Open Access) to its contents, which is likely to attract more readers and citations to articles published in ACA. Authors do not have to pay for submission, processing or publication of articles in ACA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


