{"title":"COVID-19-Induced Refractory Symptomatic Hypocalcemia in a Patient With Parathyroid Gland Reimplantation.","authors":"Crystal Tse, Ho-Man Yeung","doi":"10.1155/2024/6375828","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Several cases of severe hypocalcemia in the setting of COVID-19 have been reported. The proposed mechanisms include direct viral interaction with ACE2 receptors in the parathyroid gland, viral chelation of calcium, worsening hypovitaminosis D, critical illness leading to unbound fatty acids binding calcium, and inflammatory cytokines leading to PTH resistance. Given the life-threatening nature of hypocalcemia, this underrecognized phenomenon should be on the forefront of the clinician's attention. This case highlights a rare manifestation of COVID-19 and further complicated by the patient's reimplanted parathyroid gland. <b>Presentation:</b> A 73-year-old female with primary hyperparathyroidism status post parathyroidectomy with reimplantation in the left forearm presented with 4 days of viral syndrome, found to have tetany and Chvostek's sign on physical exam. Pertinent laboratory abnormalities included calcium 5.3 mg/dL, ionized calcium 0.44 mmol/L, magnesium 1.4 mg/dL, phosphorous 5.5 mg/dL, PTH 242 pg/mL, and 25-OH vitamin D 56 ng/mL. Chest CT revealed multifocal pneumonia consistent with positive COVID-19 testing. She was subsequently admitted to the ICU for severe, symptomatic hypocalcemia and was initiated on a continuous calcium infusion, remdesivir, baricitinib, and steroids. Tetany resolved after 9 g calcium repletion, and she was transferred to the medical floor with an ionized calcium of 0.83 mmol/L. On hospital day 3, repeat ionized calcium was 0.78 mmol/L despite ongoing repletion. Given the persistence of hypocalcemia, a repeat PTH level was obtained which remained high at 487 pg/mL, suggesting ongoing PTH interference in the setting of COVID-19. PTH was obtained from the right (nonimplanted) arm which was normal at 74 pg/mL. This indicated an appropriate PTH response from the reimplanted gland, and that ongoing hypocalcemia may be due to insufficient PTH function to maintain systemic calcium levels or a peripheral interference with PTH level. With continued calcium supplementation and treatment of COVID-19, the patient's calcium stabilized at 8.6 mg/dL. She was discharged on oral calcium supplementation with endocrinology follow-up. <b>Conclusion:</b> Acute hypocalcemia strongly correlates with a profound inflammatory response in COVID-19 patients. This case corroborates the cytokine/PTH hypothesis. This patient had a high PTH sampled near the reimplanted gland but an inappropriately normal PTH from the nonimplanted arm, indicating that direct viral interaction interfering with PTH release is an unlikely mechanism. This case represents a scenario where PTH can be sampled directly from the source and this type of model could aid in the process of determining the etiology of hypocalcemia in COVID-19.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2024 ","pages":"6375828"},"PeriodicalIF":0.9000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444793/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/6375828","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
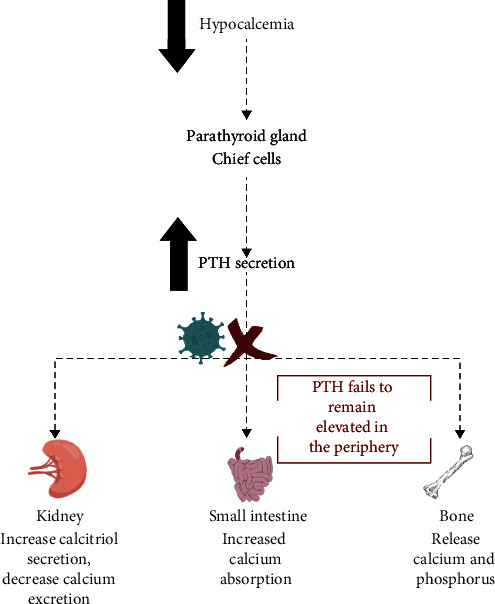
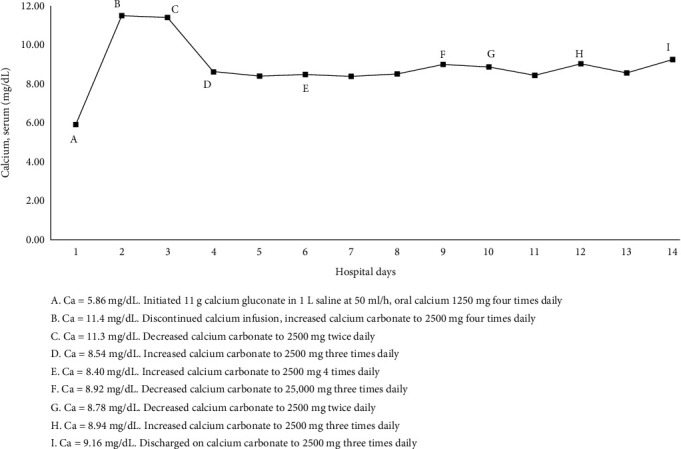
Background: Several cases of severe hypocalcemia in the setting of COVID-19 have been reported. The proposed mechanisms include direct viral interaction with ACE2 receptors in the parathyroid gland, viral chelation of calcium, worsening hypovitaminosis D, critical illness leading to unbound fatty acids binding calcium, and inflammatory cytokines leading to PTH resistance. Given the life-threatening nature of hypocalcemia, this underrecognized phenomenon should be on the forefront of the clinician's attention. This case highlights a rare manifestation of COVID-19 and further complicated by the patient's reimplanted parathyroid gland. Presentation: A 73-year-old female with primary hyperparathyroidism status post parathyroidectomy with reimplantation in the left forearm presented with 4 days of viral syndrome, found to have tetany and Chvostek's sign on physical exam. Pertinent laboratory abnormalities included calcium 5.3 mg/dL, ionized calcium 0.44 mmol/L, magnesium 1.4 mg/dL, phosphorous 5.5 mg/dL, PTH 242 pg/mL, and 25-OH vitamin D 56 ng/mL. Chest CT revealed multifocal pneumonia consistent with positive COVID-19 testing. She was subsequently admitted to the ICU for severe, symptomatic hypocalcemia and was initiated on a continuous calcium infusion, remdesivir, baricitinib, and steroids. Tetany resolved after 9 g calcium repletion, and she was transferred to the medical floor with an ionized calcium of 0.83 mmol/L. On hospital day 3, repeat ionized calcium was 0.78 mmol/L despite ongoing repletion. Given the persistence of hypocalcemia, a repeat PTH level was obtained which remained high at 487 pg/mL, suggesting ongoing PTH interference in the setting of COVID-19. PTH was obtained from the right (nonimplanted) arm which was normal at 74 pg/mL. This indicated an appropriate PTH response from the reimplanted gland, and that ongoing hypocalcemia may be due to insufficient PTH function to maintain systemic calcium levels or a peripheral interference with PTH level. With continued calcium supplementation and treatment of COVID-19, the patient's calcium stabilized at 8.6 mg/dL. She was discharged on oral calcium supplementation with endocrinology follow-up. Conclusion: Acute hypocalcemia strongly correlates with a profound inflammatory response in COVID-19 patients. This case corroborates the cytokine/PTH hypothesis. This patient had a high PTH sampled near the reimplanted gland but an inappropriately normal PTH from the nonimplanted arm, indicating that direct viral interaction interfering with PTH release is an unlikely mechanism. This case represents a scenario where PTH can be sampled directly from the source and this type of model could aid in the process of determining the etiology of hypocalcemia in COVID-19.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


